Quest for Space: Towards a Novel Approach in Treating Pain and Fatigue on Earth
International Journal of Biomechanics and Movement Science
(ISSN: 2633-8955)
Volume 2, Issue 1
Research Article
DOI: 10.35840/2633-8955/9722

Article Formats
Quest for Space: Towards a Novel Approach in Treating Pain and Fatigue on Earth
Table of Content
Figures
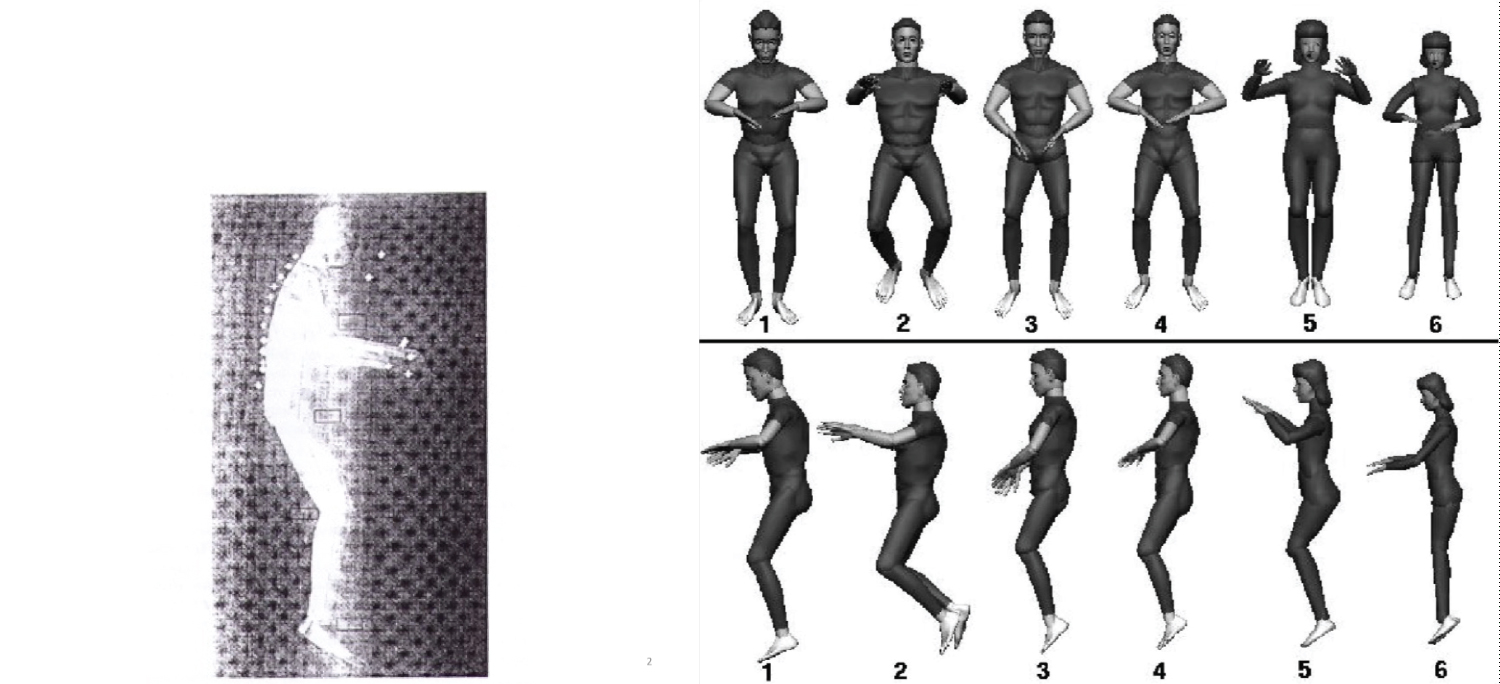
Figure 1: The microgravity's Neutral Body Position....
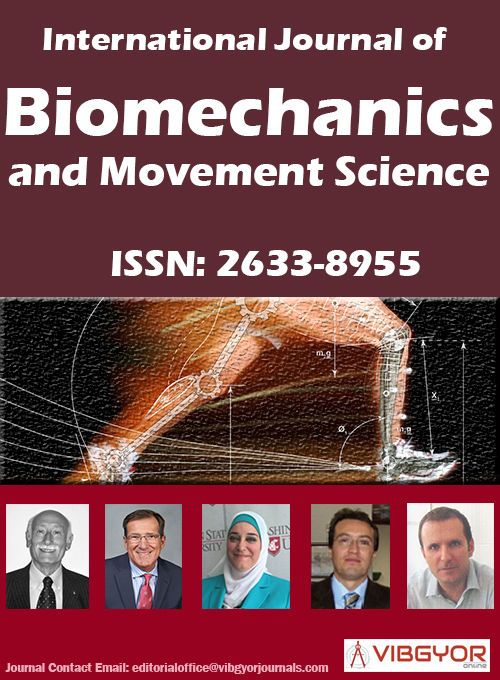
The microgravity's Neutral Body Position, a gravity-free attitude in microgravity (Left, © [53]; Right, © [54]). The astronaut's skeletal system is more akin to that of a fish in that it expands the body in all directions, less counteracted by the cabin air pressure than by water pressure.
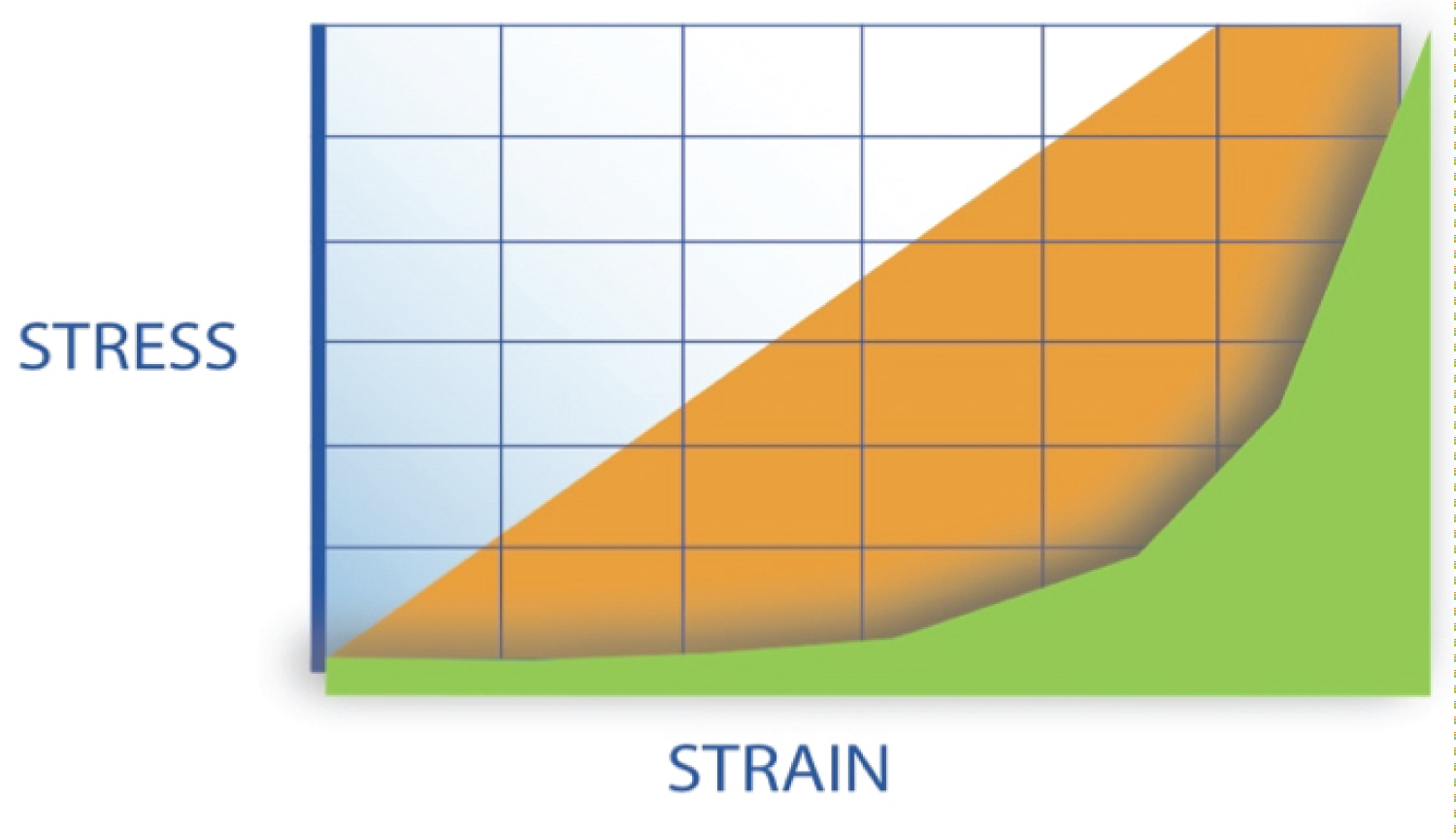
Figure 2: Stress/strain curves of brittle (orange) materials.....
Stress/strain curves of brittle (orange) materials are characterized by a straight line. Following a certain amount of strain, the material breaks. Biological materials (green) are characterized by a non-linear stress/strain curve. The graph also shows the ratio between required energy, the surface underneath both lines respectively, to achieve a specific strain (reshaping) for both kinds of material. Only at the end of the curve the biological material shows some rigidity, requiring relatively much more energy to undergo further reshaping. If used accurately, biological material may produce/undergo a lot of reshaping at the expense of a small amount of energy. The yield point divides the non-linear stress/strain curve into a left-hand and a right-hand part.
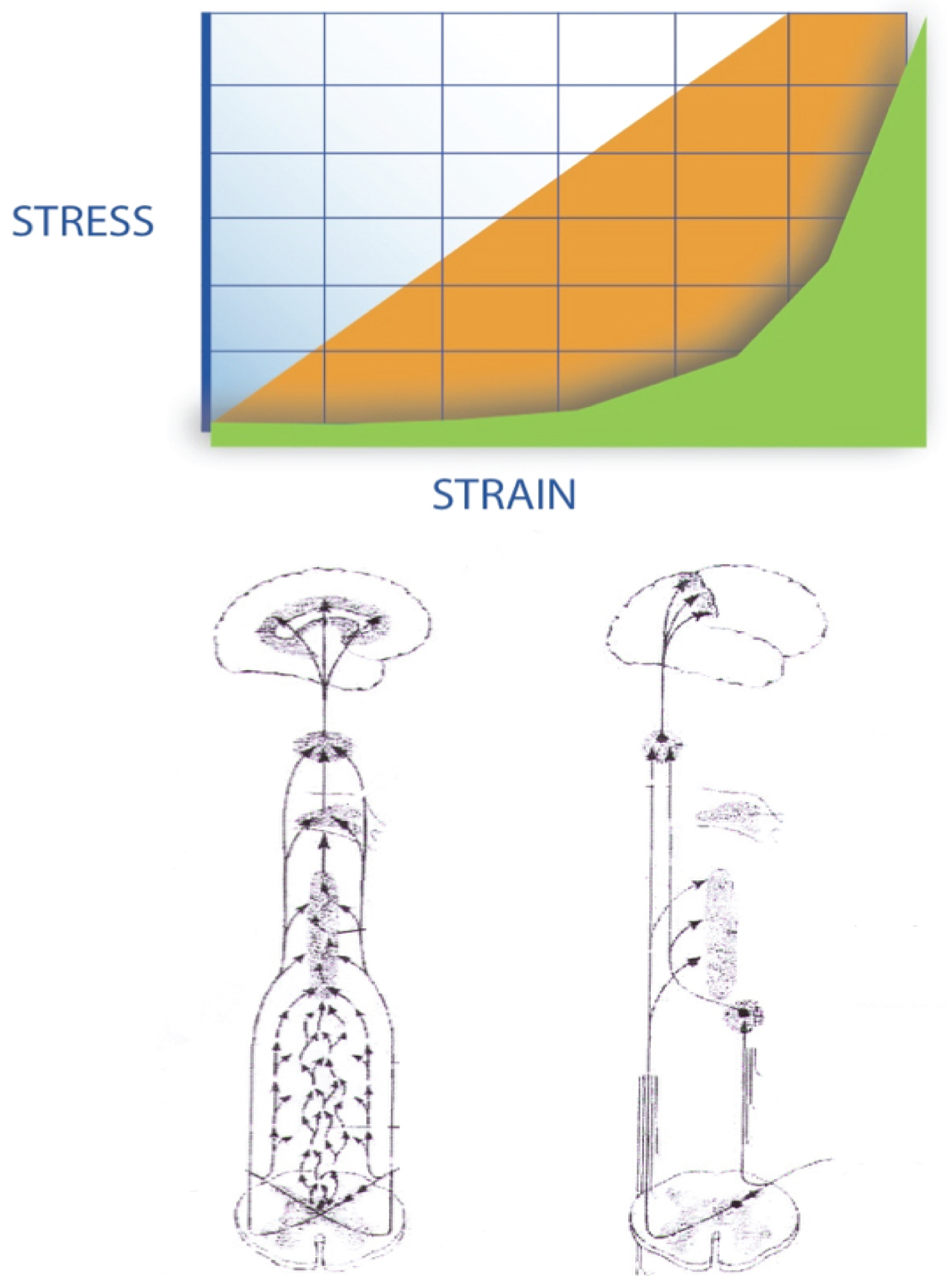
Figure 3: The motor control system uses different....
The motor control system uses different, parallel data sets in relation to the organism's surrounding and/or inner needs. Left, small-diameter type C fibers conduct afferent data over the slower tract. These fibers stimulate lateral spinothalamic tract neurons, which send collaterals into the brainstem's reticular formation, project to the thalamus and hypothalamus, giving rise to the emotional components of pain and fatigue. Pain signals following this route are poorly localized.
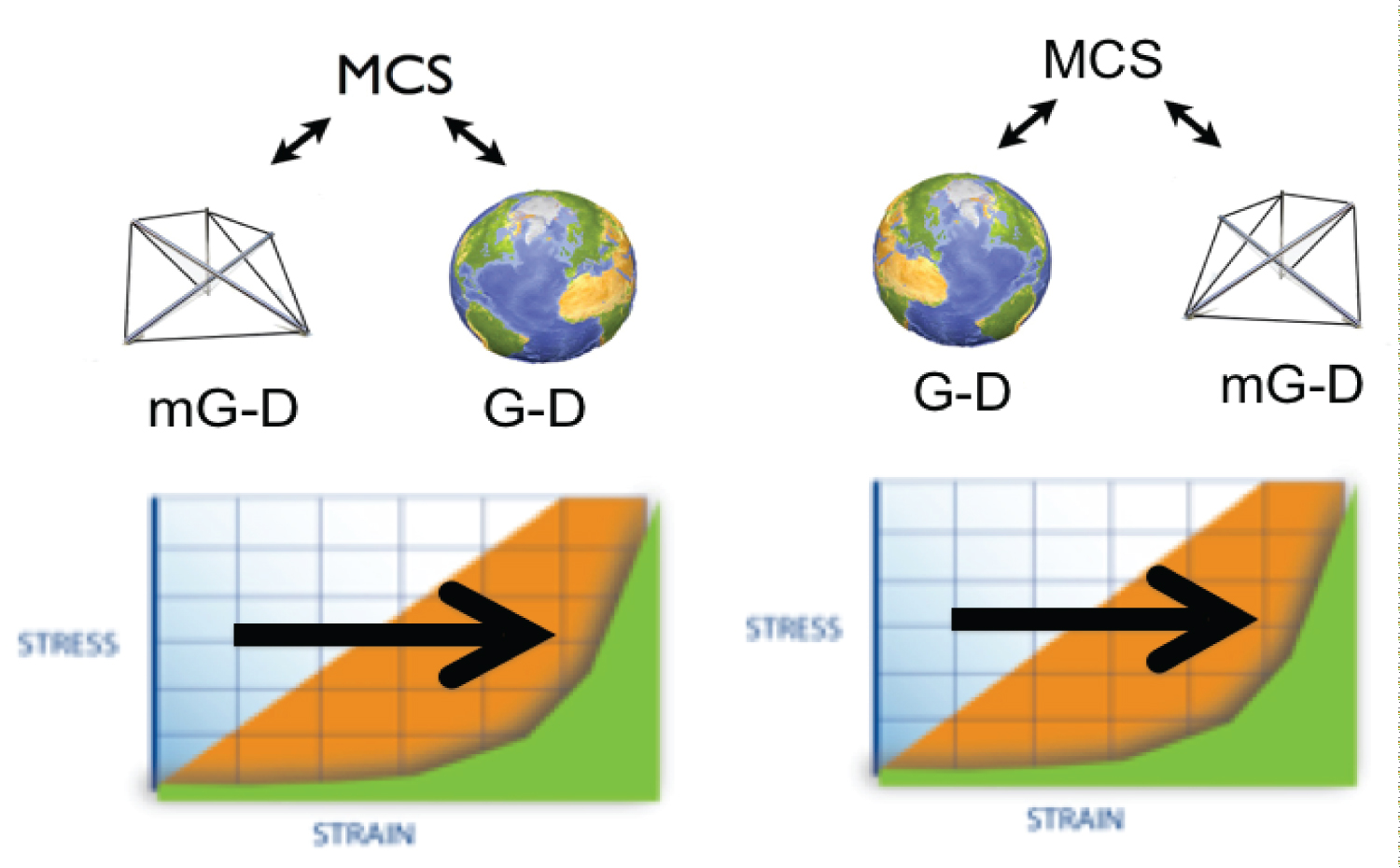
Figure 4: When being 'forced', the organism will prepare....
When being 'forced', the organism will prepare the body and/ or its parts and strains, requiring more energy. On earth, gravity dependent (G-D) and with little omni-directional counterforces (figure 4 left), or while in orbit, microgravity dependent (mG-D), lacking the predominantly vertical gravitational effect (figure 4 right), some physiological reactions stay the same. One mechanism, here coined as the motor control system (MCS) steers sensorial and motor components of the organism to allow the shift to the right-hand part of the nlSSC shift, a shift from type-1 to type-2 muscle cells.

Figure 5: Diagram of a simple lever system showing....
Diagram of a simple lever system showing that a 2 kg fish at the end of a 3 m rod would require a balancing force that would exceed the strength of the spinal muscles (reproduced with permission from © [101-103].
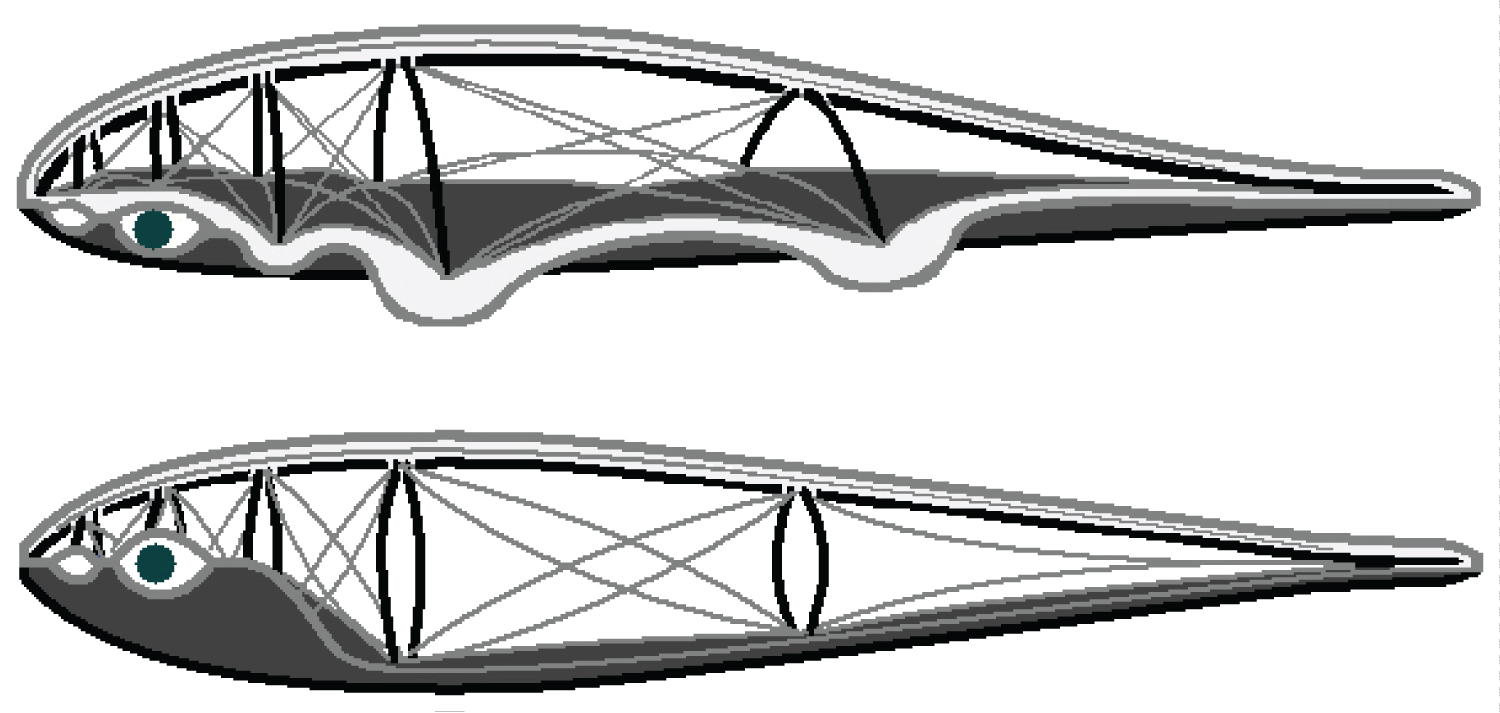
Figure 6: The musculo-skeletal system's countering....
The musculo-skeletal system's countering gravity and omni-directional forces. Take your time and try not only to 'see' the difference but also to 'feel' the difference between upper (land organism) and lower image (sea organism) (© John A. Appleton [116].
Tables
Table 1: Some physical, physiological and biological aspects related to both sides of the non-linear stress/strain curve. In real life, both extremes result in equilibrium.
Table 2: Overview of both neurological subsystems, working in parallel. The multi-synaptical is the one more related to the 'run on idle' modus of the organism, the right one to (volitional) activities. The more the fast part of the system is used; we could say 'employed', the higher the costs on the muscular and on the cerebral part.
References
- Frymoyer JW (1988) Medical progress. Back pain and sciatica. N Eng J Med 318: 291-300.
- Eyskens Jb (2000) Op zoek naar een consensusmodel voor de aanpak van rugpijn. Wetenschappelijk Tijdschrift voor Fysische Therapie 1: 21-29.
- https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions.
- Wilke J, Schleip R, Klingler W, Stecco C (2017) The lumbodorsal fascia as a potential source of low back pain: A Narrative Review. Biomed Res Int 2017: 5349620.
- Ingber DE (2008) Tensegrity-based mechanosensing from macro to micro. Progress Biophys Mol Biol 97: 163-179.
- Taguchi T, Tesarz J, Mense S (2009) The thoracolumbar fascia as a source of low back pain. In: Huijing PA, Hollander P, Findley TW, Shleip R, Fascia research II - Basic science and implications for conventional and complementary healthcare.
- Manchikanti L, Singh V, Falco FJ, Benyamin RM, Hirsch JA (2014) Epidemiology of low back pain in adults. Neuromodulation 2: 3-10.
- Pillastrini P, Gardenghi I, Bonetti F, Capra F, Guccione A, et al. (2012) An updated overview of clinical guidelines for chronic low back pain management in primary care. Joint Bone Spine 79: 176-185.
- Mannion AF (1999) Fibre type characteristics and function of the human paraspinal muscles: Normal values and changes in association with low back pain. J Electromyogr Kinesiol 9: 363-377.
- Mannion AF, Käser L, Weber E, Rhyner A, Dvorak J, et al. (2000) Influence of age and duration of symptoms on fibre type distribution and size of the back muscles in chronic low back pain patients. Eur Spine J 9: 273-281.
- Goubert D, Oosterwijck JV, Meeus M, Danneels L (2016) Structural changes of lumbar muscles in non-specific low back pain: A systematic review. Pain Physician 19: 985-1000.
- Hopker JG, Coleman DA, Gregson HC, Jobson SA, Von der Haar T, et al. (1985) The influence of training status, age, and muscle fiber type on cycling efficiency and endurance performance. J Appl Physiol 115: 723-729.
- Barclay CJ, Woledge RC, Curtin NA (2010) Inferring crossbridge properties from skeletal muscle energetics. Prog Biophys Mol Biol 102: 53-71.
- Lacour JR (2011) Muscle activity and energy expenditure from exercise physiology to medical decision. Rev Mal Respir.
- Gundersen K (1998) Determination of muscle contractile properties: The importance of the nerve. Acta Physiol Scand 162: 333-341.
- Eyskens Jb (2000) Op zoek naar een rationele revalidatie van langdurig vermoeide patie¨nten. Wetenschappelijk Tijdschrift voor Fysische Therapie 3: 17-24.
- Declercq T, Stuer H, Heytens S, Blancke S, Rogiers R, et al. (2010) De Behandeling van CVS in de eerste lijn. Uitdaging of verplicht nummer? Huisarts Nu 39: 379-384.
- Eyskens Jb, Illegems J, De Nil L, Nijs J, Kampen JK, et al. (2019) Assessing chronic fatigue syndrome: Self-reported physical functioning and correlations with physical testing. J Bodyw Mov Ther 23: 598-603.
- Cook DB, Nagelkirk PR, Peckerman A, Poluri A, Mores J, et al. (2005) Exercise and cognitive performance in chronic fatigue syndrome. Med Sci Sports Exerc 37: 1460-1467.
- Hides J, Lambrecht G, Ramdharry G, Cusack R, Bloomberg J, et al. (2017) Parallels between astronauts and terrestrial patients-Taking physiotherapy rehabilitation "To infinity and beyond". Musculoskelet Sci Pract 27: S32-S37.
- Zobel BB, Del Vescovo R, Oliva G, Russo V, Setola R (2012) Assessing bone loss in micro-gravity: A fuzzy approach. Comput Methods Programs Biomed 108: 910-921.
- Ilyin EA, Oganov VS (1989) Microgravity and musculoskeletal system of mammals. Adv Space Res 9: 11-19.
- LeBlanc AD, Spector ER, Evans HJ, Sibonga JD (2007) Skeletal responses to space flight and the bed rest analog: A review. J Musculoskelet Neuronal Interact 7: 33-47.
- Morey-Holton ER (2003) The impact of gravity on life. Evolution on planet earth: The impact of the Physical Environment, 143-159.
- Belavy DL, Adams M, Brisby H, Cagnie B, Danneels L, et al. (2016) Disc herniations in astronauts: What causes them, and what does it tell us about herniation on earth? Eur Spine 25: 144-154.
- Bailey JF, Miller SL, Khieu K, O'Neill CW, Healey RM, et al. (2018) From the international space station to the clinic: How prolonged unloading may disrupt lumbar spine stability. Spine J 18: 7-14.
- Mulder T (2001) De geboren aanpasser, over beweging, bewustzijn en gedrag. Uitgeverij Contact, Amsterdam, Netherlands.
- Hargens AR, Richardson S (2009) Cardiovascular adaptations, fluid shifts, and countermeasures related to space flight. Respir Physiol Neurobiol 169: S30-S33.
- Chopard A, Hillock S, Jasmin BJ (2009) Molecular events and signalling pathways involved in skeletal muscle disuse-induced atrophy and the impact of countermeasures. J Cell Mol Med 13: 3032-3050.
- Hargens AR, Bhattacharya R, Schneider SM (2013) Space physiology VI: Exercise, artificial gravity, and countermeasure development for prolonged space flight. Eur J Appl Physiol 113: 2183-2192.
- Booth FW, Criswell DS (1997) Molecular events underlying skeletal muscle atrophy and the development of effective countermeasures. Int J Sports Med 18: S265-S269.
- Droppert PM (1993) A review of muscle atrophy in microgravity and during prolonged bed rest. J Br Interplanet Soc 46: 83-86.
- Yoshinobu O (2000) Neuromuscular adaptation to microgravity environment. Japanese Journal of Physiology 50: 303-314.
- Ingalls CP (2004) Nature vs nurture: Can exercise really alter fiber type composition in human skeletal muscle? J Appl Physiol 97: 1591-1592.
- Talavrinov VA, Anashkin OD, Bagramov KhG, Volgin VA, Luk'ianchikov VI (1988) Anthropometric studies of crewmembers of Salyut-6 and Salyut-7. Kosm Biol Aviakosm Med 22: 22-27.
- Antonutto G, di Prampero PE (2003) Cardiovascular deconditioning in microgravity: Some possible countermeasures. Eur J Appl Physiol 90: 283-291.
- Shenkman BS (2016) From slow to fast: Hypogravity-induced remodeling of muscle fiber myosin phenotype. Acta Naturae 8: 47-59.
- Talbbot J, Maves L (2016) Skeletal muscle fiber type: Using insights from muscle developmental biology to dissect targets for susceptibility and resistance to muscle disease. WIREs Developmental Biology 5: 518-534.
- Horowitz JF, Sidossis LS, Coyle EF (1994) High efficiency of type I muscle fibers improves performance. Int J Sports Med 15: 152-157.
- Purves-Smith FM, Sgarioto N, Hepple RT (2014) Fiber typing in aging muscle. Exerc Sport Sci 42: 45-52.
- Bollinger LM (2017) Potential contributions of skeletal muscle contractile dysfunction to altered biomechanics in obesity. Gait Posture 56: 100-107.
- Edgerton VR, McCall GE, Hodgson JA, Gotto J, Goulet C, et al. (2001) Sensorimotor adaptations to microgravity in humans. J Exp Biol 204: 3217-3224.
- Wostyn P, De Deyn PP (2017) Intracranial pressure-induced optic nerve sheath response as a predictive biomarker for optic disc edema in astronauts. Biomark Med 11: 1003-1008.
- Wostyn P, De Winne F, Stern C, De Deyn PP (2018) Dilated prelaminar paravascular spaceurtins as a possible mechanism for optic disc edema in astronauts. Aerosp Med Hum Perform 189: 1089-1091.
- Alperin N, Bagci AM (2018) Spaceflight-induced visual impairment and globe deformations in astronauts are linked to orbital cerebrospinal fluid volume increase. Acta Neurochir 126: 215-219.
- Leone G, Lipshits M, Gurfinkel V, Berthoz A (1995) Influence of graviceptives cues at different level of visual information processing: The effect of prolonged weightlessness. Acta Astronaut 36: 743-751.
- Krafczyk S, Knapek M, Philipp J, Querner V, Dieterich M (2003) Optokinetic stimulation in microgravity: Torsional eye movements and subjective visual vertical. Aviat Space Environ Med 74: 517-521.
- Mechtcheriakov S, Berger M, Molokanova E, Holzmueller G, Wirtenberger W, et al. (2002) Slowing of human arm movements during weightlessness: The role of vision. Eur J Appl Physiol 87: 576-583.
- Kornilova LN, Naumov IA, Azarov KA, Sagalovitch VN (2012) Gaze control and vestibular-cervical-ocular responses after prolonged exposure to microgravity. Aviat Space Environ Med 83: 1123-1134.
- Clarke AH, Schönfeld U (2015) Modification of unilateral otolith responses following spaceflight. Exp Brain Res 233: 3613-3624.
- Vieira S, Quercia P, Bonnetblanc F, Michel C (2013) Space representation in children with dyslexia and children without dyslexia: Contribution of line bisection and circle centering tasks. Res Dev Disabil 34: 3997-4008.
- Mount FE, Whitmore M, Stealey SL (2003) Evaluation of neutral body posture on shuttle mission STS-57 (SPACEHAB-1). NASA TM-2003-104805.
- Souvestre PA, Landrock CK, Blaber AP (2008) Reducing incapacitating symptoms during space flight: Is postural deficiency syndrome an applicable model? Hippokratia 12: 41-48.
- Andreoni G, Rigotti C, Baroni G, Ferrigno G, Colford NAT, et al. (2000) Quantitative analysis of neutral body posture in prolonged microgravity. Gait and Posture 12: 235-242.
- Smith SM, Krauhs JM, Leach CS (1997) Regulation of body fluid volume and electrolyte concentrations in spaceflight. Adv Space Biol Med 6: 123-165.
- Lacquaniti F, Ivanenko YP, Sylos-Labini F, La Scaleia V, La Scaleia B, et al. (2017) Human locomotion in hypogravity: From basic research to clinical applications. Front Physiol 8: 893.
- Vernazza-Martin S, Martin N, Massion J (2000) Kinematic synergy adaptation to microgravity during forward trunk movement. J Neurophysiol 83: 453-464.
- Rapoport DL (2011) On the fusion of physics and klein bottle logic in biology, embryogenesis and evolution. NeuroQuantology 9: 842-861.
- Tafforin C (1994) Synthesis of ethological studies on behavioural adaptation of the astronaut to space flight conditions. Acta Astronaut 32: 131-142.
- Cassady K, Koppelmans V, Reuter-Lorenz P, De Dios Y, Gadd N, et al. (2016) Effects of a spaceflight analog environment on brain connectivity and behavior. Neuroimage 141: 18-30.
- Reschke MF, Cohen HS, Cerisano JM, Clayton JA, Cromwell R, et al. (2014) Effects of sex and gender on adaptation to space: Neurosensory systems. J Womens Health (Larchmt) 23: 959-962.
- Balcetis E, Dunning D (2006) See what you want to see: Motivational Influences on visual perception. J Pers Soc Psychol 91: 612-625.
- Clément G (2007) Using your head: Cognition and sensorimotor functions in microgravity. Gravitational and Space Biology 20: 65-78.
- Graebe A, Schuck EL, Lensing P, Putcha L, Derendorf H (2004) Physiological, pharmacokinetic, and pharmacodynamic changes in space. J Clin Pharmacol 44: 837-853.
- Irons-Brown S, Jones SM, Jones TA (2000) A putative role for the cerebellum in avian vestibular responses to linear translation. ASGSB.
- Thornton W, Moore T (1987) Height changes in microgravity. In: Bungo MW, Bagian TM, Bowman MA, Levitan BM, Results of the life sciences DSOs conducted aboard the space shuttle 1981-1988. NASA, Johnson Space Center, Houston, USA, 55-57.
- Wing PC, Tsang IK, Susak L, Gagnon F, Gagnon R, et al. (1991) Back pain and spinal changes in microgravity. Orthop Clin North Am 22: 255-262.
- Fuchs HS (1980) Man in weightlessness: Physiological problems, clinical aspects, prevention and protection. Related Bio-medical research in microgravity during the forecoming SPACELAB missions. Riv Med Aeronaut Spaz 43: 332-346.
- Melzack R (1976) Pain measurement and assessment Raven Press, New York.
- Styf JR, Hutchinson K, Carlsson SG, Hargens AR (2001) Depression, mood state, and back pain during microgravity simulated by bed rest. Psychosomatic Medicine 63: 862-864.
- Yamamoto N, Otsuka K, Kubo Y, Hayashi M, Mizuno K, et al. (2015) Effects of long-term microgravity exposure in space on circadian rhythms of heart rate variability. Chronobiol Int 32: 327-340.
- Lipnicki DM, Gunga HC, Belavy DL, Felsenberg D (2009) Decision making after 50 days of simulated weightlessness. Brain Res 1280: 84-89.
- Berry CA (1973) Effects of weightlessness in man. Life Sci Space Res 11: 187-199.
- Stampi C (1994) Sleep and circadian rhythms in space. J Clin Pharmacol 34: 518-534.
- Vigo DE, Ogrinz B, Wan L, Bersenev E, Tuerlinckx F, et al. (2012) Sleep-wake differences in heart rate variability during a 105-day simulated mission to Mars. Aviat Space Environ Med 83: 125-130.
- Barger LK, Flynn-Evans EE, Kubey A, Walsh L, Ronda JM, et al. (2014) Prevalence of sleep deficiency and use of hypnotic drugs in astronauts before, during, and after spaceflight: An observational study. Lancet Neurol 13: 904-912.
- Rai B, Foing BH, Kaur J (2012) Working hours, sleep, salivary cortisol, fatigue and neuro-behavior during mars analog mission: Five crews study. Neurosci Lett 516: 177-181.
- Borelli GA (1680) De Motu Animalium.
- Tian Y, Ding L, Liu H, Li Y, Li D, et al. (2016) Effects of EVA gloves on grip strength and fatigue under low temperature and low pressure. Appl Ergon 53: 17-24.
- Ferrando AA, Paddon-Jones D, Wolfe RR (2002) Alterations in protein metabolism during space flight and inactivity. Nutrition 18: 837-841.
- Mannion AF, Dumas GA, Stevenson JM, Cooper RG (1998) The influence of muscle fiber size and type distribution on electromyographic measures of back muscle fatigability. Spine 23: 576-584.
- Vanhatalo A, Black MI, DiMenna FJ, Blackwell JR, Schmidt JF, et al. (2016) The mechanistic bases of the power-time relationship: Muscle metabolic responses and relationships to muscle fibre type. J Physiol Aug 594: 4407-4423.
- Pietrangelo T, Toniolo L, Paoli A, Fulle S, Puglielli C, et al. (2009) Functional characterization of muscle fibres from patients with chronic fatigue syndrome: Case-control study. Int J Immunopathol Pharmacol 22: 427-436.
- Yunus MB, Kalyan-Raman UP, Kalyan-Raman K, Masi AT (1986) Pathologic changes in muscle in primary fibromyalgia syndrome. Am J Med 81: 38-42.
- Henriksson KG (1988) Muscle pain in neuromuscular disorders and primary fibromyalgia. Eur J Appl Physiol Occup Physiol 57: 348-352.
- Melzack R, Wall PD (1965) Pain mechanisms, a new theory. Science 150: 971-979.
- Travell JG, Simons DG (1998) Travell and simon's myofascial pain and dysfunction. (2nd edn), Lippincott Williams and Wilkins, Revised edition, Philadelphia, Pennsylvania, USA.
- Schleip R, Klingler W (2019) Active contractile properties of fascia. Clinical Anatomy 32: 891-895.
- Mcgilchrist I (2009) The master and his emissary: The divided brain and the making of the western world. Yale University Press.
- LaMotte C (1977) Distribution of the tract of Lissauer and the dorsal root fibers in the primate spinal cord. J Comp Neurol 172: 529-561.
- Jang SH, Kwon HG (2013) Anatomical location of the medial lemniscus and spinothalamic tract at the pons in the human brain: A diffusion tensor tractography study. Somatosens Mot Res 30: 206-209.
- Selye H (1973) The evolution of the stress concept: The originator of the concept traces its development from the discovery in 1936 of the alarm reaction to modern therapeutic applications of syntoxic and catatoxic hormones. Sigma Xi, The Scientific Research Honor Society 61: 692-699.
- Martinez-Lavin M, Infante O, Lerma C (2008) Hypothesis: The chaos and complexity theory may help our understanding of fibromyalgia and similar maladies. Semin Arthritis Rheum 37: 260-264.
- Kurz MJ, Stergiou N, Bloomberg J, Miller D (2005) Does gravity influence the structure of chaotic gait patterns? ISB XXth Congress - ASB 29th Annual Meeting, Cleveland, Ohio.
- Wegner DM (2003) The mind's best trick: How we experience conscious will. Trends in Cognitive Sciences 7: 65-69.
- Libet B (1985) Unconscious cerebral initiative and the role of conscious will in voluntary action. Behavioral and Brain Sciences 8: 529-566.
- Hagg GM (1989) Zero crossing rate as an index of electromyographic spectral alterations and its applications to ergonomics. Rheumatic Disease Clinics of North America.
- Eyskens Jb, Nijs J, D'Aou^t K, Sand A, Wouters K, et al. (2015) Timed loaded standing in female chronic fatigue syndrome compared with other populations. Journal of Rehabilitation Research & Development 52: 21-29.
- Eyskens Jb, Nijs J, Wouters K, Moorkens G (2015) Reduced gait automaticity in female patients with chronic fatigue syndrome: Case-control study. Journal of Rehabilitation Research & Development 52: 805-814.
- Frost HM (2004) A 2003 update of bone physiology and Wolff's law for clinicians. Angle Orthod 74: 3-15.
- Scarr G (2018) Biotensegrity: The structural basis of life, (2nd edn). Edinburgh, Handspring.
- Delp SL, Suryanarayanan S, Murray WM, Uhlir J, Triolo RJ (2001) Architecture of the rectus abdominis, quadratus lumborum and erector spinae. Journal of Biomechanics 34: 371-375.
- Hansen L, de Zee M, Rasmussen J, Anderson TB, Wong C, et al. (2006) Anatomy and biomechanics of the back muscles in the lumbar spine with reference to biomechanical modeling. Spine 31: 1888-1899.
- Sharkey J (2016) Biotensegrity-Fascia and the fallacy of biomechanics. Parts 1,2,3. AAMT J.
- Sharkey J (2018) Biotensegrity-anatomy for the 21st century. Informing yoga and physiotherapy concerning new findings in fascia research. Journal of Yoga and Physiotherapy, 6.
- Ingber DE (2003) Mechanobiology and diseases of mechanotransduction. Annals of Medicine 35: 564-577.
- Sharkey J (2019) Regarding: Update on fascial nomenclature-an additional proposal by John Sharkey MSc, clinical anatomist. Journal Bodywork and Movement Therapies 23: 6-8.
- Caspar D, Klug A (1962) Physical principles in the construction of regular viruses. Cold Spring Symp Quant Biol 27: 1-24.
- Levin S, Martin DC (2012) The mechanics of fascia. In: Schleip, Findley, Chaitow, Huijing, FASCIA: The Tensional Network of the Human Body. Elsevier, Edinburgh, Scotland.
- Levin SM (1981) The icosahedron as a biologic support system. Houston: Alliance for Engineering in Medicine and Biology.
- Levin SM (1982) Continuous tension, discontinuous compression, a model for biomechanical support of the body. Bulletin of Structural Integration, Rolf Institute, Bolder, 31-33.
- Levin SM (1987) Theories about spinal loading. Spine 12: 422-423.
- Simons DG, Dommerholt J (2004) Myofascial pain syndromes-trigger points. Journal of Musculoskeletal Pain 12: 57.
- Chaitow L, DeLany J (2003) Neuromuscular techniques in orthopedics. Tech Orthop 18: 74-86.
- Appleton JA (2007) Illustrations and mental imagery of archetypal forms of early organisms-a new approach to exposing and releasing habitual and dysfunctional posture. Journal of Bodywork and Movement Therapies 11: 25-36.
- Sharkey J (2008) Concise book of neuromuscular therapy: A trigger point manual. North Atlantic Press, Berkley California.
- Marr D, Nishihara HK (1978) Representation and recognition of the spatial organisation of three-dimensional shapes. Proceedings of the Royal Society London B 200: 269-294.
- Marr D (1982) Vision: A computational investigation into the human representation and processing of visual information. WH Freeman, New York, USA.
- Biederman I (1995) Visual object recognition. In: Kosslyn SM, Osherson DN, An invitation to cognitive science, Visual cognition and action, Cambridge Mass, MIT press, 2.
- Gatt R, Vella Wood M, Gatt A, Zarb F, Formosa C, et al. (2015) Negative poisson's ratios in tendons: An unexpected mechanical response. Acta Biomater 24: 201-208.
- Baker CE (2011) Auxetic spinal implants: Consideration of negative poisson's ratio in the design of an artificial intervertebral disc. Thesis, The University of Toledo.
- Hullegie W (2016) Oplossingsruimte als indicator voor de gezondheid van het bewegingsapparaat. Anders kijken naar motoriek en bewegen. Fysiopraxis.
- Brown A (1993) Circumnutations: From darwin to space flights. Plant Physiol 101: 345-348.
- Eyskens Jb (2007) Body in peace. Antwerpen, Standaard Uitgeverij, Belgium.
- Nijs J, Meeus M, Heins M, Knoop H, Moorkens G, et al. (2012) Kinesiophobia, catastrophizing and anticipated symptoms before stair climbing in chronic fatigue syndrome: An experimental study. Disability and rehabilitation 34: 1299-1305.
- Heins M, Knoop H, Nijs J, Feskens R, Meeus M, et al. (2012) Influence of symptom expectancies on stair-climbing performance in chronic fatigue syndrome: Effect of study context. International Journal of Behavioral Medicine 20: 213-218.
- Eyskens Jb (2019) Eye-scans, a deck of cards.
- Rothenberg B, Rothenberg O (1995) Touch training for strength. Human Kinetics, Champaign, IL, USA.
- Cyriax H (1904) The elements of kellgrens manual treatment. W Wood and Co, New York.
- Staring J (2005) Frederick matthias alexander 1869-1955. Integraal (Werkgroep Integrerende Wetenschapsbeoefening), Nijmegen, The Netherlands.
- Quercia P, Seigneuric A, Chariot S, Bron A, Creuzot-Garcher C, et al. (2007) Étude de l'impact du contrôle postural associé au port de verres prismatiques dans la réduction des troubles cognitifs chez le dyslexique de développement. Journal Français d'Ophtalmologie 30: 380-389.
- Godts D, Moorkens G, Mathysen DG (2016) Binocular vision in chronic fatigue syndrome. Am Orthopt J 66: 92-97.
- Sharkey J (2015-2020) Biotensegrity focused thiel soft fixed dissection course. Department of Anatomy and Human Identification, College of Life Sciences, University of Dundee, Scotland.
- Nijs J, Meeus M, Van Oosterwijck J, Ickmans K, Moorkens G, et al. (2012) In the mind or in the brain? Scientific evidence for central sensitization in chronic fatigue syndrome. Eur J Clin Invest 42: 203-212.
- Eyskens Jb, De Nil L, Staring J (2020) A tool to reorient physiotherapy: The use of the field model. Ann Anesth Pain Med 3: 1007.
Author Details
Jan B Eyskens1*, John J Sharkey2, John A Appleton3, Luc De Nil4 and Jeroen Staring5
1Department of Internal Medicine, Antwerp University Hospital, Belgium
2MSc Clinical Anatomy, MSc Exercise Physiology, Department of Medicine, Dentistry and Clinical Sciences University of Chester/NTC, Dublin Ireland
3Certified Teacher of the Alexander Technique, USA
4MSc Science in Physiotherapy and Rehabilitation, Belgium
5Dr. Medical Sciences, Dr. Pedagogy, MSc Anthropology, Master SEN, Master Education, BA Mathematics, Unaffiliated Independent Researcher, Schin op Geul, The Netherlands
Corresponding author
Jan B Eyskens, Department of Internal Medicine, Antwerp University Hospital, Belgium.
Accepted: December 12, 2020 | Published Online: December 14, 2020
Citation: Eyskens JB, Sharkey JJ, Appleton JA, Nil LD, Staring J (2020) Quest for Space: Towards a Novel Approach in Treating Pain and Fatigue on Earth. Int J Biomech Mov Sci 2:002
Copyright: © 2020 Eyskens JB, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
On earth so-called mechanical body overload, causing tissue strain, tissue damage and fatigue, is considered to be a major cause of physical complaints including neck and lower back pain. Mechanical strain related to body posture has been shown to play a significant role in ongoing, widespread pain and fatigue (patients prefer to lie down while limiting standing and sitting). Understandably, the link to gravity's vertical vector is quickly made.
The authors felt it would be an interesting question to ask, "What would happen to pain and ongoing fatigue when in orbit, in a micro-gravity environment, lacking the earth's dominating vertical vector?"
Surprisingly, results show that in micro-gravity both pain and fatigue are found occurring frequently. Data obtained from a literature review regarding both complaints in microgravity provides evidence for a change of perspective. This review's focus, confined to type-1 and type-2 muscle fiber type, highlighted a shift in muscle physiology specific to astronauts when in a microgravity environment. A similar shift in muscle fiber physiology among chronic low back patients and patients suffering from chronic fatigue syndrome exists on earth.
It is proposed that biomechanics, as commonly implemented and interpreted based on levers, might be better informed by including a concept based on biotensegrity. This could be used to propose novel therapeutic approaches to address both local, regional and widespread pain as well as ongoing fatigue.
Keywords
Back pain, Biotensegrity, Chronic fatigue syndrome, Chronic pain, Fibromyalgia, Microgravity, Muscle fiber types, Fascia
Introduction
Research informs us that in Western societies, musculo-skeletal disorders constitute a costly medical condition [1,2]. In 2019 the World Health Organization identified low back pain as being the single leading cause of disability globally [3].
In more recent years a plethora of fascia research [4] has revealed the dense innervation of the thoracolumbar fascia replete with free nerve endings including nociceptive afferents. An identified essential role of the fascia is the sharing and translating of forces generated by the muscle fibers, this process is known as "mechanotransduction" [5]. It seems reasonable to assume that physiological changes in type-1 and Type-2 muscle fibers would lead to morphological change as described in fascia research [6]. The frequency of low back pain in a general adult population has a point prevalence of approximately 12%, with a one-year prevalence of 38%, and a lifetime prevalence of approximately 40% [7]. In 90% of the patients, the etiology of the pain remains obscure [4]. Despite the continuation of research and therapeutic interventions, the incidence of low back pain and the associated costs, financial and economical, on society continue to rise [8].
A significant percentage of people affected with pain become chronic [8]. Chronic pain is associated with modification from type-1 to type-2 muscle cells [9-11]. This modification is related to the efficiency of function [12], which on a local level has been described for type-1 muscle fibers [13]. Consequences for the use of the body as a whole must ensue [14] including physiological adaptations to the nervous system [15].
In chronic conditions such as widespread pain and/or fatigue a diagnosis as fibromyalgia syndrome (FMS) or chronic fatigue syndrome (CFS) [16-18] can be used when specific criteria are met [19]. Since parallels exist between terrestrial patients and astronauts in orbit experiencing pain and fatigue, the key role of gravity can be brought into question [20]. In addition, an interesting observation concerns the growth of bones in microgravity. Bone growth is equivalent to bone growth on earth regarding length, but not regarding girth. Regarding girth, bone growth is reduced. In microgravity, it has been demonstrated that bones lose material due to reduced 'stress' on the body as a whole [21].
A noticeable inhibition of osteogenesis has been observed in astronauts by the third week in orbit [22]. Space flights of more than six months cause such a large reduction of the load-bearing capacity of bone that LeBlanc, et al. suggest that a higher frequency of fractures can be expected to occur in an astronaut's life in older age [23]. After a safe return to earth, the incidence of fractures due to osteoporosis remains high [24]. Intervertebral disks show a higher risk of herniation [25]. A combination of effects leads to spinal degeneration [26]. It has been proposed that gravity does not substantially influence the actions carried out by the smooth muscle tissue [27] or striated cardiac muscle [28]. Mulder [27] suggests that strictly distinguishing between 'movement' muscles and 'postural' muscles is not possible and not advisable. During flights, some countermeasures concerning osseofascial pain and fatigue are intensively used as a preventative measure [29,30].
A global view of muscle
Global muscular atrophy results due to the absence of imposed load in microgravity, even after short space flights [31]. A reduction of up to 37% in muscle mass has been observed after only one week [32]. Reported muscle loss values range from 11 to 24% after only five days [31]. Atrophy begins in extensor muscles and after six months it appears in flexor muscles [33]. Atrophy, and the general medical condition of astronauts is, to a certain extent, related to the intensity of appropriate physical activities/exercise during flight rather than to the total time spent in space [34]. Crewmembers in most space flights experience a body weight drop of 1.2 up to 6.0 kilograms. In some, however, an increase (1.0 up to 4.5 kilograms) has been observed [35]. In flights between five and seven days, structural and metabolic modifications in the nerve/ muscle excitation contraction link were noticed. Antonutto suggests that microgravity causes a fundamental change in motor control [36].
Impacts on type-1 and type-2 muscle fibers
Newer categorizations of muscle fibers have recently been described to include type-I, type-IC, type-2C, type-2AC, type-2A, type-M and type-2X, however they are generally classified as being either slow-twitch type-1 or fast-twitch type-2 muscle fibers [37,38]. Type-1 fibers react more rapidly than type-2, due to their smaller motor neurons, yet they contract more slowly [39]. Type-1 fibers work within an aerobic environment and function mainly during slow movements where they do not suffer oxygen depletion. Hence, they are coined 'posture' controlling muscles [11,40,41].
The lack of gravity on the eyeball leads to morphological changes and neural dynamics required to estimate one's position in the surrounding space [42]. After long-duration space flights, visual impairment, eye globe deformations [43,44] and optic disc oedema have been noted [45].
Lack of graviceptive cues has its consequences [46], especially for the positioning of the eyes in the skull [47], and additional consequences such as decelerating the functions of the upper limbs [48]. Gaze control [49] and its coordination with vestibular-cervical reflexes [50] will have an influence on body form and its functions [51].
Microgravity's neutral body form-referred to as "Neutral Body Position" (NBP)-is depicted in Figure 1 [52]. NBP resembles the underwater body form. This has specific influences on the body's functioning and can lead to a 'postural deficiency syndrome' [53].
In microgravity, human length increases six to eight centimeters. Astronauts are taller than the tallest measurements taken on earth in the morning. The spinal column is lengthened mainly by the diminished lumbar and cervical lordosis, but also by the increase of the inter-vertebral spaces. Interestingly, these findings are taken into account when designing cockpits [54]. Redistribution of blood leads to remarkable changes in the overall body form. For example, the commonly called 'puffy face' involving the swelling of the head as compared to earth conditions and 'bird legs' involving the diminishing of the volume of the lower limbs [55].
Astronauts use the same kinematic synergy for the hip, knee, and ankle articulations when bending forward from an 'upright' position in microgravity [56]. The forward/backward movement of their center of mass proves to be restricted to a minimum in microgravity. Nevertheless, electromyography, suggests that another muscular specific body segment/inertia strategy is used. In 2000, Vernazza-Martin, et al. [57] informed us that the central nervous system uses a top-down regulating strategy to minimize the forward/ backward and lateral center of mass displacements, using an internal, embodied system, independent of information from otoliths or other body graviceptors. This may influence muscle fiber selection and functions towards type-2 muscle cells, with the possibility of creating a double recursive loop described in 2011 by Rapoport as the Klein Bottle Logic [58].
Depending on various parameters, a partial adaptation of behavior is possible [59] related to brain connections [60]. Gender and cultural differences also play a role related to the adaptation to specific space environment [61]. Moving a hand to produce a horizontal 'Figure 1' is disturbed during parabolic flights when compared to normogravity. When catching a thrown object in microgravity, the brain mistakenly anticipates the effect of gravitation [62]. Clément explained in 2007 that an object is expected to arrive 'lower' than it actually does and that astronauts look reflexively 'down' if an object 'drops' from their hands [63].
Next to Space Motion Sickness, back pain and fatigue are the two most frequent complaints of astronauts during flights [64]. After the fourth day of flight, most processes return to what astronauts describe as 'functional normality', mainly because of substitution of vestibular data by neck receptor data [65]. Back pain is one of the most frequently occurring medical problems during space flight having been reported by 68% of astronauts [66] [67]. Seventy-two percent of shuttle crew members experienced one or other forms of back pain. 28% of complaints were moderate to 'severe' [68]. Duration of pain varied from 14% to 100% of flight time, increasing the potential to seriously jeopardize a crewmember's performance when in orbit.
The intensity of the pain was measured using a 10-cm visual analogue scale [69] between 2:00 and 3:00 PM daily [70]. Being in orbit influences astronauts' circadian rhythms [71] and decision-making [72]. When in orbit, fatigue is related to sleep complaints, due to the disappearance of normal parameters such as day length, normally related to sunlight [73,74]. The autonomic system also adapts its reactivity [75], influencing both sleep patterns [76] and fatigue [77]. Local fatigue has been measured and is in relation to grip strength [78].
Parallel Dysfunctions on Earth and in Microgravity
As in space so on earth [79], a shift from type-1 to type-2 fibers is established in adult patients suffering from chronic low back pain [80], fatigue [81], chronic fatigue syndrome (CFS) [82], fibromyalgia syndrome (FMS) [83,84].
Material qualities of biological materials are characterized by non-linear stress-strain curves (nlSSC). In biological tissue, as in Figure 2, reshaping starts at a point known as the yield point. Increased load is needed to further strain/deform the tissue. At even higher loads, biological material tears apart, causing sprains or fractures.
According to the 1965 dual gate theory of pain espoused by Melzack and Wall [85] when we move or function in a rash way, our biological material becomes strained. It has been further proposed that this is due to our neurological system, in turn having consequences for the system as a whole [86]. Larger motor units, connected to type-2 muscle cells, using fewer synapses, will then be put into action. It has been reported that the body feels as if it is stiffening and is thought of as being anisotropic [87]. The left-hand side of the nlSSC is used when functioning in a 'run on idle' modus, being properly poised, functioning in a skilled way. When this left-hand part of the curve becomes dominant using multi-synaptic nerve fibers and energy efficient T1 muscle cells, we judge our functioning as being efficient; we feel relaxed and energetic.
Table 1 gives an overview of the different aspects of both parts of the nlSSC.
The relationship between moving with our three-dimensional bodies in a three-dimensional space (either in normogravity or in microgravity) and our two-dimensional thinking mainly with our left hemisphere, even its relationship with our Western culture, has been a topic of much debate [88].
On a lower level, the spinal cord, it is widely accepted that the left-hand part of the nlSSC relates more to multi-synaptic information (see Figure 3). The afferent part of the information is related to the postero-lateral tract as described by Lissauer (1861-1891) [89], centrally projecting its axons carrying discriminative pain and temperature information. These sensory data enter the spinal column to ascend or descend one or two spinal segments in this tract, before penetrating the grey matter of the dorsal horn where they synapse on second-order neurons. These data do not reach the brain cortex. The efferent part, the fusimotor system (small gamma motor neurons located in the brainstem and spinal cord) controls and modifies muscle spindle sensitivity to provide proprioceptive feedback concerning position and the form of limbs or parts of the body. This steering component is related to the body form as a whole and to steering slow reshaping preferably using type-1 muscle cells. The right part of the nlSSC uses fewer synapses.
On the afferent side, the axons (fine, mostly non-myelinated slow fibers) cross the midline to join the spinothalamic tract. Their synapses connect to neurons located in the thalamus and they do reach the cortex. The efferent part, the extrafusal system from skeletal muscles (larger alpha motor neurons located in brainstem and spinal cord), initiates (voluntary) muscle contraction linked to (voluntary) movements and egomotion.
The faster right tract is using type A delta fibres over the lateral spinothalamic tract fibers, which travel to the thalamus on the contralateral side. From here third order fibers project to the cerebral cortex where they are somatotopically organized [90].
Based on accepted neurophysiology and neuro-cognitive behavior the authors suggest the definitions set out in Table 2 with each afferent part of the steering mechanism having distinct properties related to different sub-functions of living organisms.
Different Environments, Similar Complications
Selye, in 1936, introduced to the world the concept of 'stress'. Selye overruled this term four years later, stating that he should have, more appropriately, used the term 'strain'. Prolonged strain did lead to a 'stress reaction' with effects that could become stressors and thereby maintaining a vicious circle [91].
Healthy systems are characterized by chaotic behavior, producing more coherent interactions than less healthy ones [92]. Control of this chaotic behavior reduces the need for continuous recalculation [93]. When actually needed, this asks for fast and forceful reactions-using more T2 muscle fibers - entailing an even larger shift to the right-hand side of the nlSSC with even larger energy expenditure. When this way of functioning becomes a habit, the anticipation for daily activities will be primed by less ergonomically and energetically based procedures being ready for type-2 muscle cells. Wegner, summarizing Libet's work, explained this non-habitual way of thinking as follows: A movement starts with qualities well before the mover is aware of the movement [94,95] (Figure 4).
When all this 'employment' is only needed for merely a short period of time and followed by returning to 'run on idle' modus, the recovery can begin. If, on the contrary, the process of straining takes too long, degradation will follow. Nevertheless, complaints of back pain, on-going widespread pain and fatigue seem to occur when organisms do not function in a 'run on idle' modus but have shifted towards an 'employment' mode for short heavy physical load or for longstanding uninterrupted low load conditions, either on earth [96] or in microgravity. Antonutto's 2003 observation [36] that microgravity causes a fundamental change in motor control can be considered as a meta-statement concerning other changes reported in this review [97].
From Borelli's Classical Biomechanics towards Levin's Biotensegrity
Since Giovanni Borelli's time (1608-1679), movement is understood as a product of shortening of muscles when contracting and hence pulling bones that are viewed as levers. In his concept gravity plays a crucial role [98]. Borelli's lever concept is used to treat patients [99] with acute and chronic conditions such as back pain, FM and CFS. These patients often find relief by lying down or slumping in chairs in an effort to seek support. Sitting or standing without support (i.e. counteracting gravity's vertical vector) increases their complaints. Following Wolf's law for the most part biological structures are just as materially strong as they need to be to perform their particular function because they do not need to be stronger [100]. In Borelli's biomechanics, however, the idea of 'levers' leads to the miscalculation of forces at the fulcrum.
Calculated mechanical forces at the fulcrum suggest biological material to be much stronger than it actually is, as the next Figure 5 demonstrates.
In Figure 5 [101-103] the supposition is that Borelli's lever/fulcrum classical mechanics model does not take into account internal mechano-transductive forces depending on functions of the body as a whole and in various regions and tissues [104]. It is suggested that this concerns a 2D concept, whereas tensegrity concerns a more realistic 3D concept [105]. This comes down to the difference between pure classical mechanics versus biomechanics taking into account concepts of mechano-transduction forces in the body [106]. It not only concerns the pure calculus of assumed Borelli influenced mechanical forces but includes internal physiological forces of various interplaying interdependent tissues as well [107]. Understanding tensegrity could provide novel insights into former, rather mechanical, insights of the shifting balances between self-destructing forces and self-reconstructing capabilities, in for example osseo-fascial regeneration processes after complicated fractures [101].
Biotensegrity, no need for levers or fulcrums
The 1962 Caspar/Klug theory [108] proposed a synergy between virus structures and geodesic domes. Fuller, who coined the term tensegrity, and Snelson, who first applied the mechanical principles to modern structures as an art form, have conceived 'Tensegrity' as a concept. All of these authors refer to Fuller's original definition: "The word tensegrity is an invention: A contraction of tension and integrity". It is important to note that forces emerging in a tensegrity system are omni-directional [109]. The particularity of a tensegrity structure is based on the synergy between components of compression (e.g., struts or bones) and components of tension (e.g., tensile structures, muscles, fascia). Tensegrities and living tissues both display auxetic characteristics, expanding and contracting in multiple directions, i.e. they show a negative Poisson effect. This way, due to compression, expansion is possible, outward from the structure as a whole. During the early 1980s, Ingber described the fundamental design of cells: "Cells use tensegrity architecture to organize their cytoskeleton and stabilize their form" [5,106]. Levin coined the term 'Biotensegrity', describing the living relationship between biomechanics and tensegrity [110,111]. On earth, Levin wondered, "What pulls us up?" [112]. Others cite tensegrity as a mechanism involved in musculo-skeletal pain, a problem affecting mainly type-2 muscle fibers [86,113,114].
From an evolutionary point of view, the neurological model for musculo-skeletal support, movement, and expression from archetypal forms in early organisms has been kept similar during evolution as described by Appleton [115]. Since life and its body plans started under water, the original structures had to counter the omni-directional pressure similar to the embryonic environment where the skeletal system is formed within the first eight weeks of embryology [116].
In Figure 6 we are presented with an example of Postural Release Imagery (PRI) by Appleton [116]. Although Figure 6 is a two-dimensional (2D) image, it invites us to implement 'depth'. This is needed to feel the difference between the upper and the lower image with our three-dimensional (3D) bodies and our 3D governed right hemisphere [88].
This change of concept has important consequences for medicine, movement and physical therapies. It facilitates a differing view to Borelli's lever system [98], still used as the basic mechanical theory for therapists to explain body posture, movement and its disorders as well as to explain the approaches used in remediation [117-119].
Linear thinking and 3 dimensionality
Recently, evidence was found of biological material behaving in a 3D manner, behaving in an auxetic manner. Gatt, et al. [120] demonstrated in 2015 that tendons, essential for positioning of the body in space as well as for energy storing when involved in abrupt movements, exhibit a negative Poisson's ratio. These tissues expressed auxetic qualities in some planes when stretched up to 2% along their length. This report is backed by in vivo and ex vivo experiments in humans' as well as in sheep and pigs' Achilles tendons. The same fundamentals underpin the search for materials to be used in lumbar disk prostheses, having a negative Poisson's ratio and offering the 3D compression/expansion qualities as described by Baker in 2011 having auxetic properties [121].
According to Mcgilchrist, as we are thinking about our actions, our attention drifts to the right-hand part of the nlSSC, and to the left hemisphere [88]. This relates to the fact that the purpose of functioning is related to the right-hand, straining part of the nlSSC, particularly when force and speed are involved. On the other hand, when actions are related to the left-hand part of the nlSSC, it regards slow reshaping and subtle movements. Actions seldom require continuous attention, unless they are prolonged and uninterrupted, or require very forceful intervention at which point discomfort emerges. As a consequence, it has been proposed that our movements are felt and rationally conceived as 'lever-like' (thus 2D), especially by (chronic) patients since moving has become difficult, demanding specific attention. When this way of functioning persists in time, it influences our believes and influences our way of thinking, a part of acquired 'bad habits' [122].
Discussion with recommendations for further research
Discussions on the nature and influence of gravity on movement are not new. In 1875 Darwin described how climbing plants changed their form while growing. Darwin called the process 'circumnutation' and was of the opinion that its driving forces were unrelated to gravity. Many years later, research on board space crafts has provided evidence to support Darwin's sharp observations and thesis [123].
The authors of this article hope it can be understood in a meaningful way as to support the long over-due shift from a linear to a non-linear concept and model, from a 2D to a 3D body perspective and from a body of parts towards a more comprehensive whole-body approach [124].
A change in quality, rather than a change in quantity of movement seems then to be indispensable. The focus of this research paper specifically concerned the influence of gravity as one vector to be considered in the etiology and pathophysiology of low back pain and fatigue in micro and normo-gravity environments.
Researchers should also consider investigating additional possible influencing factors such as consequences of DNA deterioration/regeneration due to, for instance, radiation or circadian rhythm. Following our findings, the authors would like to propose a policy directed at influencing the habitual afferent neuro-muscular data, at least in a subgroup of patients with dysfunctional strategies [125,126]. When patients with chronic back pain, FM and/or CFS have a need to change their habits, their skills and/ or their poise, specific cues are required to 'prime' their right hemisphere [127].
As research suggests we are not hard-wired to make a deliberate shift to the left-hand part of the nlSSC, specific cues will be needed if we wish to be congruent with Libet's fundamental findings [91]. Being 'autopoietic' living organisms, cues needed to fundamentally change one's habits (at least at the beginning of the rehabilitation program) must come from the outside of the body [128], that is, from the guiding hands of a skilled therapist before the patient can make use of them on their own [58,124].
Touch training and manual therapies outlined by Kellgren were used to influence the movement patterns and velocities of patients for the better [129]. In touch training an outsider gently provides the specific cue (i.e. feedback) to the organism as a whole to help it return to surmount the physio-logical cut [58], one example is the technique developed by Mathias Alexander [130]. Further research is needed to implement recent knowledge regarding correction of vision and of posture to minimize mechanical strain in the body [131,132]. Regarding microgravity conditions, the authors recommend additional research to underpin the concept of biotensegrity to measure whether astronauts do not only lengthen, but also widen and 'deepen' when in space. Research departments having expertise in biomechanics and embryology could perform bespoke dissections as have been done since 2015 at Dundee University, department of anatomy and human identification in Scotland [133]. Following the first historic dissection with a focus on the model of biotensegrity, research has been directed to investigate principles of a biotensegrity model, including investigations into the accuracy of articulating cartilage acting as a shock absorber [133]. In addition, we suggest that investigating mental stress as a contributing factor for pain and fatigue in astronauts would be an excellent topic for future research.
Conclusion
On earth, and in microgravity, organisms, subject to the 2nd law of thermodynamics, minimize their energy expenditure. The 'final' human body plan is to achieve an upright posture. This suggests that humans are hard-wired to function upright when in a gravitational field. The author's aim was to investigate if an alternative model for explaining human movement, as opposed to the classical Borelli levers and fulcrum system, could help to explain why the same physical complaints occur on earth and in a microgravity environment such as in orbit. We hope this review of space related literature will lead to a paradigm shift away from levers and fulcrums to a movement towards a new proposed model of living tensegrity. In an effort to provide effective therapeutic interventions to the growing population of individuals in industrialized societies suffering from back pain, chronic widespread pain and on-going fatigue, we suggest novel strategies should be developed and implemented [134], using specific cues influencing the way patients move, and not exclusively prescribing and adjusting the amount of movements. Results could be compared with the habitual results as mentioned in the guidelines.
How to move then becomes the primary target of the rehabilitation strategy, rather than how much to move. Quality precedes quantity, efficiency precedes strength. The authors stress that such a program should be performed with a strict engagement, that it has to be coded, and that the patient's context should offer the possibilities needed in such a way that the patient has the option to implement the changes in their daily life [135].