International Journal of Optics and Photonic Engineering
(ISSN: 2631-5092)
Volume 3, Issue 2
Research Article
DOI: 10.35840/2631-5092/4510

Article Formats
Oxygen Saturation of Dorsiflexor Muscles during Sustained Isometric Contraction
Table of Content
Figures
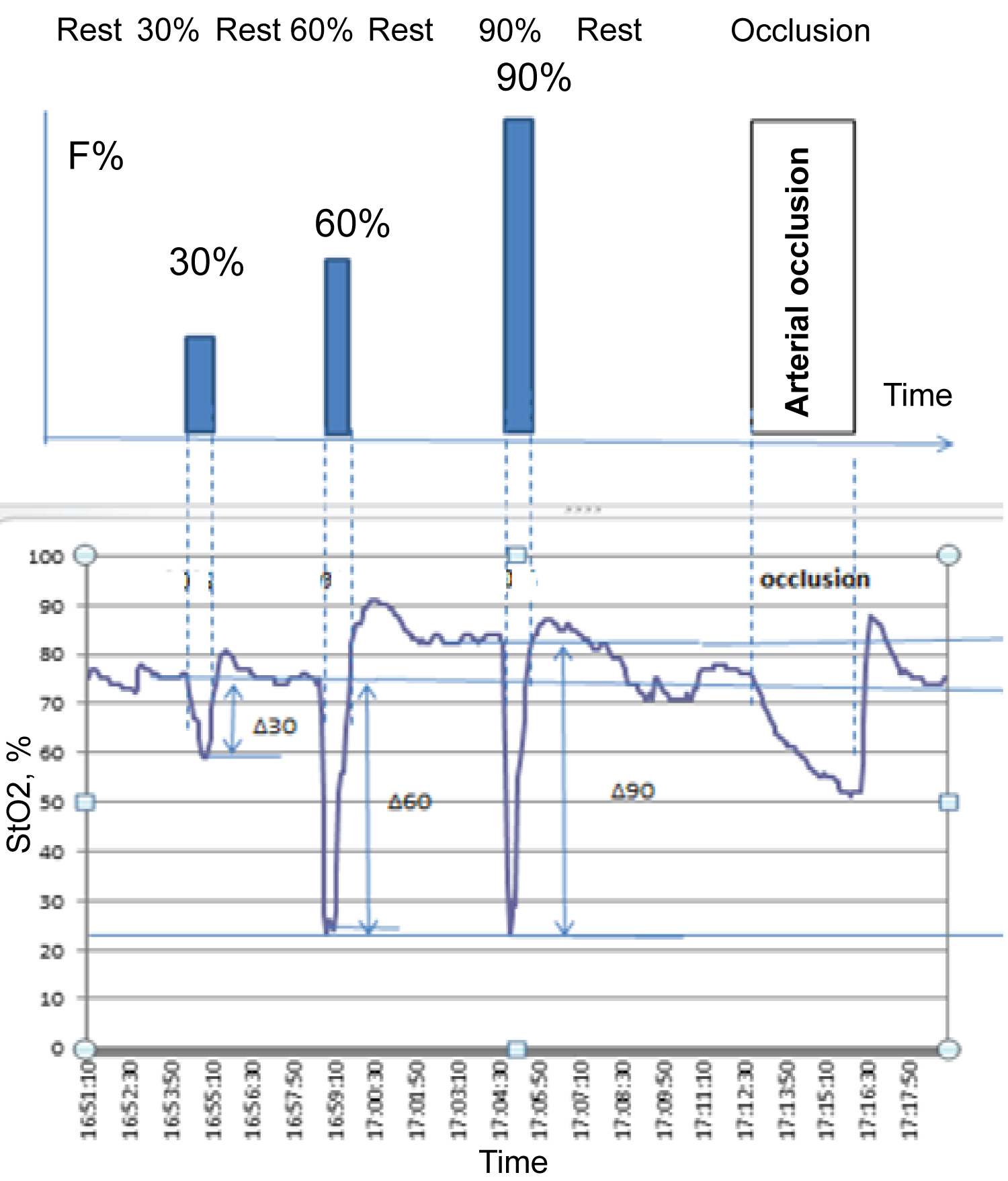
Figure 1: Protocol of experiment (top) and example of StO2 trace...
Protocol of experiment (top) and example of StO2 trace (bottom). During moderate and submaximal SIC, subjects were not able to perform the exercise for one whole minute.
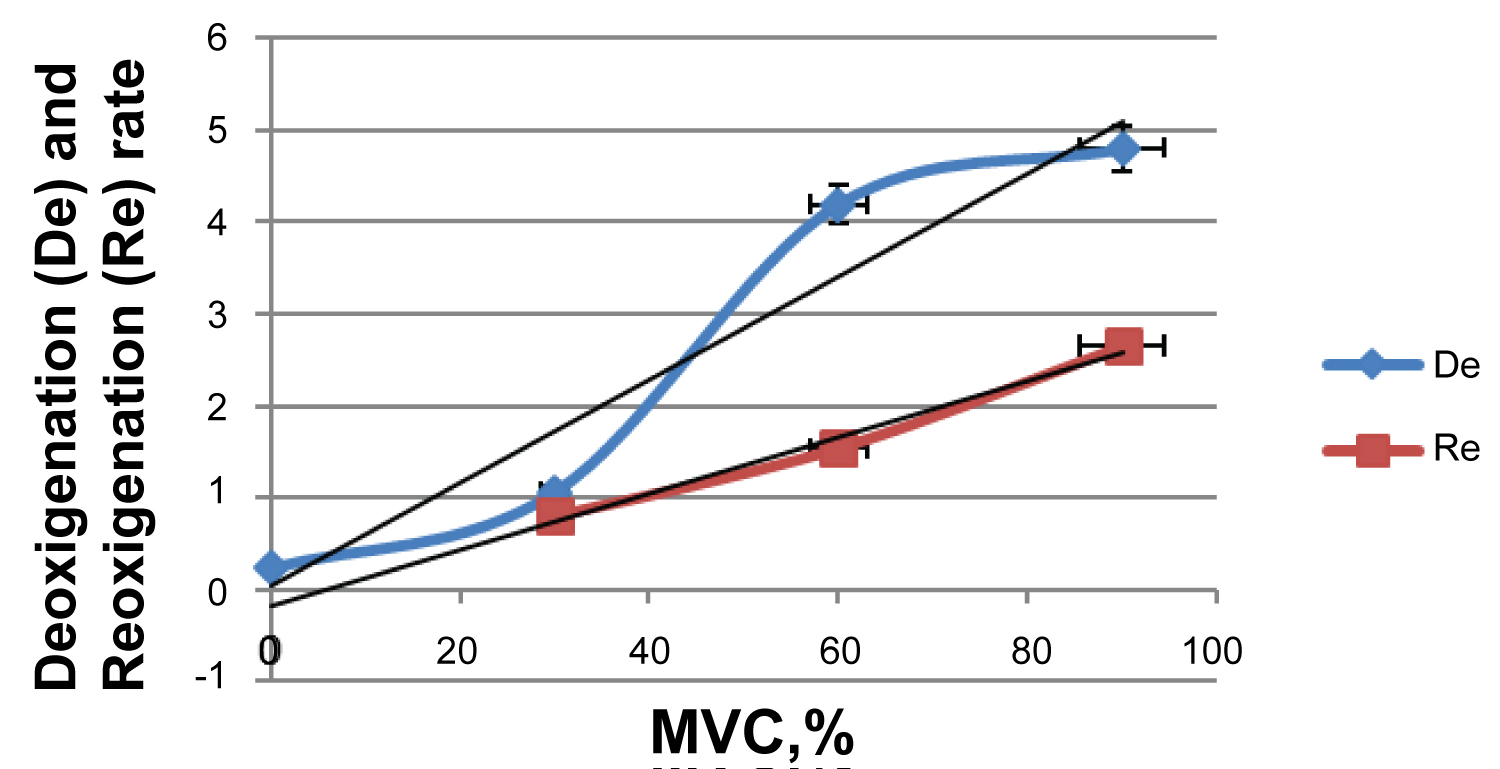
Figure 2: Deoxygenation and reoxygenation rate depend on the intensity...
Deoxygenation and reoxygenation rate depend on the intensity of the sustained isometric contraction. MVC = Percent of maximal voluntary contraction.
Tables
Table 1: Muscle StO2 parameters during sustained isometric contractions and arterial occlusion (AO). F = Force; RB = Baseline during rest; PB = Performance baseline; De = Desaturation rate during contraction and AO; Re = Resaturation rate after contraction and AO; ∆StO2 = Difference between rest and minimum during contraction and AO. Values in mean ± SD.
References
- Degens H, Salmons S, Jarvis JC (1998) Intramuscular pressure, force and blood flow in rabbit tibialis anterior muscles during single and repetitive contractions. Eur J Appl Physiol Occup Physiol 78: 13-19.
- Saltin B, Radegran G, Koskolou MD, Roach RC (1998) Skeletal muscle blood flow in humans and its regulation during exercise. Acta Physiol Scand 162: 421-436.
- Chris J McNeil, Matti D Allen, Eric Olympico, J Kevin Shoemaker, Charles L Rice (2015) Blood flow and muscle oxygenation during low, moderate, and maximal sustained isometric contractions. Am J Physiol Regul Integr Comp Physiol 309: 475-481.
- Sjogaard G, Savard G, Juel C (1988) Muscle blood flow during isometric activity and its relation to muscle fatigue. Eur J Appl Physiol Occup Physiol 57: 327-335.
- Vollestad NK, Wesche J, Sejersted OM (1990) Gradual increase in leg oxygen uptake during repeated submaximal contractions in humans. J Appl Physiol 68: 1150-1156.
- Wesche J (1986) The time course and magnitude of blood flow changes in the human quadriceps muscles following isometric contraction. J Physiol 377: 445-462.
- Hughson RL, Shoemaker JK, Tschakovsky ME, Kowalchuk JM (1996) Dependence of muscle VO2 on blood flow dynamics at onset of forearm exercise. J Appl Physiol 81: 1619-1626.
- M Wolf, M Ferrari, V Quaresima (2007) Progress of near-infrared spectroscopy and topography for brain and muscle clinical applications. J Biomed Opt 12: 062104.
- T Hamaoka, KK McCully, V Quaresima, K Yamamoto, B Chance (2007) Near-infrared spectroscopy/imaging for monitoring muscle oxygenation and oxidative metabolism in healthy and diseased humans. J Biomed Opt 12: 062105.
- Vasiliki Gerovasili, Stavros Dimopoulos, Georgios Tzanis, Maria Anastasiou-Nana, Serafeim Nanas (2010) Utilizing the vascular occlusion technique with NIRS technology. International Journal of Industrial Ergonomics 40: 218-222.
Author Details
Adkham Paiziev* and Fikrat Kerimov
Uzbekistan State Institute of Physical Culture, Tashkent, Uzbekistan
Corresponding author
Adkham Paiziev, Uzbekistan State Institute of Physical Culture, Tashkent, Uzbekistan.
Accepted: August 11, 2018 | Published Online: August 13, 2018
Citation: Paiziev A, Kerimov F (2018) Oxygen Saturation of Dorsiflexor Muscles during Sustained Isometric Contraction. Int J Opt Photonic Eng 3:010.
Copyright: © 2018 Paiziev A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Sustained isometric contractions of skeletal muscles produce intramuscular pressures that lead to blood flow restriction. Thus, we have the paradox of rising O2 demand due to muscle activity and at the same time reduced blood flow. Aim: To assess muscle oxygenation during sustained isometric low (30%), moderate (60%) and submaximal (90% of maximal voluntary contraction (MVC)) contraction of the dorsiflexor muscle. Experiments were conducted on the dominant (right) leg of 8 male students of Uzbekistan State Institute of Physical Culture (age: 19 ± 2 years, weight: 75 ± 6 kg). Tissue oxygen saturation (StO2) was recorded from the tibialis anterior using near-infrared spectroscopy. StO2 was higher at 30% compared to both 60% and 90% MVC at all time points after the start of the exercise and higher at 60% than 90%. This indicates that the supply of O2 did not keep up with its consumption. During an arterial occlusion the minimal StO2 reached 24 ± 1.77%, which is significantly higher than StO2 during 60% and 90% MVC. After each contraction there was a large and immediate hyperaemic response, whose resaturation rate continuously increased from 30% to 60% to 90% MVC. The StO2 resaturation rate was positively correlated with the MVC, indicating a vasodilation depending on the intensity of the exercise.
Introduction
Sustained isometric contraction (SIC) of skeletal muscles produces intramuscular pressure that restricts muscle blood flow (MBF) and limits O2 delivery to tissue [1]. MBF plays a key role in regulating the intensity and type of muscle contractions [2]. A limited MBF due to SIC leads to fatigue due lack of O2 and nutrients. Thus, we have the paradox of rising O2 demand due to muscle activity and at the same time reduced MBF. To clarify this issue much research has been performed mainly on MBF [3-6]. But during exercise there are few measurements of MBF by Doppler ultrasound. Although MBF could be measured by fMRI and PET, this is not possible during training [7].
Previous studies indicate that complete occlusion of MBF occurs at 50-60% of maximal voluntary contractions (MVC) during SIC [3,4,6]. MBF was not occluded at the level of the conduit artery during any of the contraction intensities [3]. Some studies report insensitivity of MBF to the muscle contraction intensity. Thus, our understanding of the oxygenation of the skeletal muscle in response to different intensities of SIC (low, moderate, submaximal MVC) still remains limited.
Despite advantages of fMRI, PET and Doppler ultrasound only one paper has been partly devoted to measure the hemodynamic response of muscles to SIC [3] by near infrared spectroscopy (NIRS). In the near-infrared spectrum (700-900 nm) light penetrates deeply into the tissue and oxyhemoglobin and deoxyhemoglobin are the strongest absorbers, while myoglobin (Mb) absorbs less. NIRS is an established optical technique to monitor concentration changes of oxyhemoglobin, deoxyhemoglobin, total hemoglobin and tissue oxygen saturation (StO2) in a variety of tissues [8,9]. NIRS instruments are non-invasive, small, and applicable in exercise physiology studies.
The aim was to assess changes in muscle oxygenation during of low, moderate and submaximal SIC of the dorsiflexor muscle.
Methods
The dorsiflexor muscle was selected, because both venous outflow and arterial inflow can be occluded by a proximal cuff. Without blood supply, the muscle metabolism depends on the O2 in capillaries and muscle cells. Consequently, the oxyhemoglobin and StO2 decrease, while deoxyhemoglobin increases and total hemoglobin remains constant. After the occlusion a hyperemic response occurs, i.e. a rapid increase in oxyhemoglobin, total hemoglobin and StO2, while deoxyhemoglobin is washed-out. From this procedure, we calculated O2 consumption, reoxygenation rate and the half-recovery times of the signals [10].
The recovery baseline (RB) value is the StO2 value after stabilisation during the rest period following a test period. The performance baseline is the minimum StO2 value reached during SIC.
Student's t-test was used to compare StO2, desaturation rate and resaturation rate at slow, moderate and submaximal MVC. All data were analyzed using the statistical software package "Statistica" for Windows (version 13). Statistical significance was set at 0.05.
Results
Figure 1 displays a typical measurement in one subject. PB decreased from low to moderate to submaximal SIC30% MVC (Table 1). Figure 2 compares the StO2 traces for different intensities of SIC. StO2 was higher at low compared with both moderate and submaximal MVC (P < 0.05) at all time points after the start of the exercise and higher at moderate than submaximal MVC (p < 0.05). Desaturation rate (De, Table 1) increased from slow (30%) to moderate (60%) to submaximal contractions (p < 0.05). Trends of De as a function of MVC are shown in Figure 2. After each contraction there was a large and immediate hyperemic response (Figure 1). The resaturation rate (Re) of StO2 after SIC depends on the intensity of the SIC and reflects the integrity and functionality of vascular system. It corresponds to a blood vessel vasodilation in response to the SIC. Re increased from slow to moderate (p < 0.05) but remained similar for moderate to submaximal SIC (Table 1 and Figure 1).
During the arterial occlusion the minimal StO2 was 52% (Table 1 and Figure 1), which is significantly higher than StO2 after moderate or submaximal SIC.
Conclusion
• The sharp decreases in StO2 after the start of moderate and submaximal SIC, indicates that the blood vessels are occluded due to intramuscular pressure. This indeed shows that O2-delivery is impeded and cannot cope with the increased O2-consumption.
• StO2 resaturation rate (Re) permanently increased from low to moderate to submaximal contractions. This reflects the resaturation of haemoglobin, which depends on integrity and functionality of vascular system and reflects blood vessel vasodilation.
Acknowledgement
The authors express their gratitude to the Swiss National Science Foundation to support this work via grant no. IZ74Z0_137423 (S-84301-05-01).