International Journal of Atomic and Nuclear Physics
(ISSN: 2631-5017)
Volume 5, Issue 1
Original Article
DOI: 10.35840/2631-5017/2519

Article Formats
Routine Care and Maintenance of Harshaw 6600 Plus (TLD) Reader in the Personnel Dosimetry Laboratory in Radiation Protection Institute in Ghana
Table of Content
Figures
Figure 1: Showing picture of Harshaw TLD....
Showing picture of Harshaw TLD 6600 Plus Reader output.


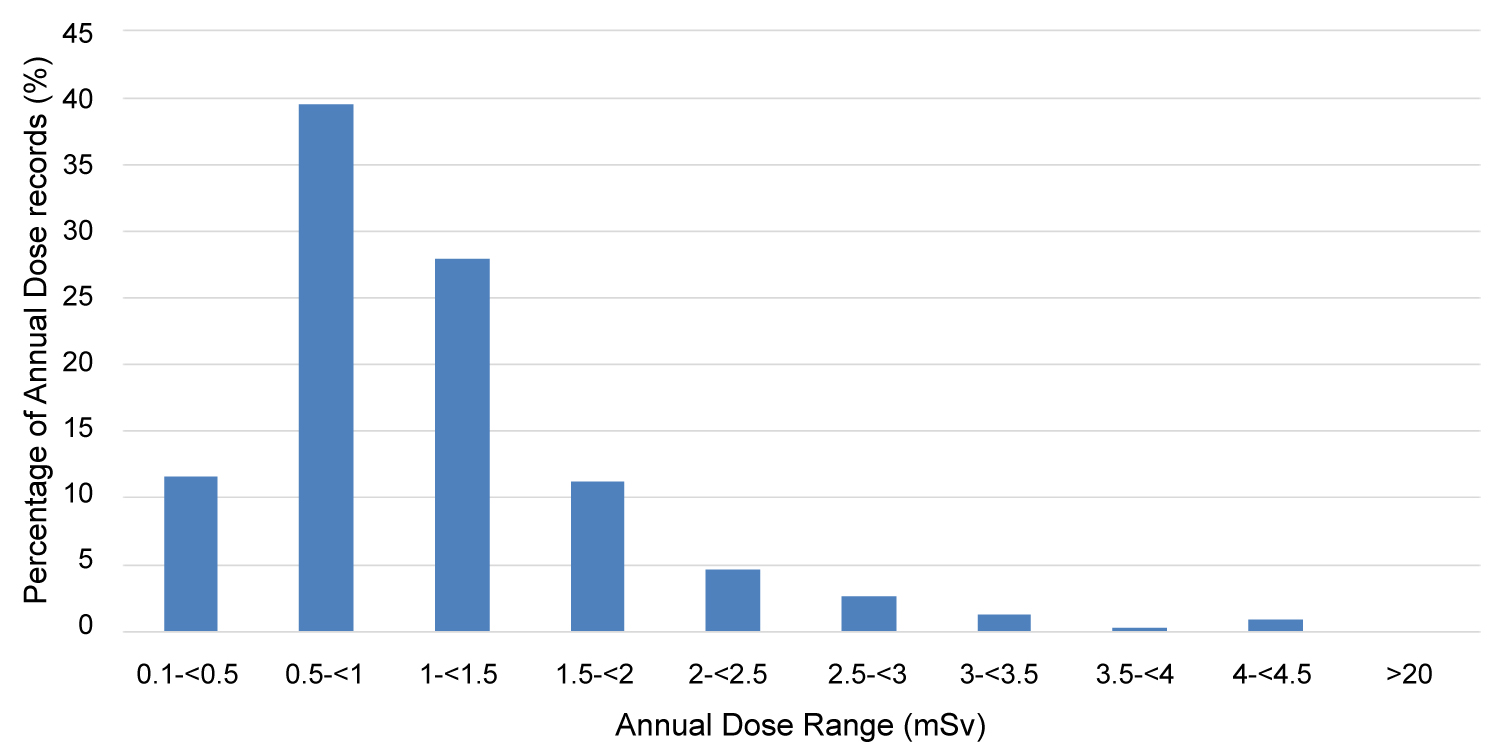
Figure 4: Dose distribution of annual dose.....
Dose distribution of annual dose records from 2011-2015.
Tables
Table 1: Format the average annual effective dose.
Table 2: Format the annual collective dose and percentage contribution of subgroups.
Table 3: Format the various electronic QC parameters on Harshaw TLD 6600 Plus reader.
References
- Attix FH (1986) Introduction to radiological physics & radiation dosimetry. John Wiley & Sons, Canada.
- Colgan PA, Currivan L, Fenton D (2008) An assessment of annual whole-body occupational radiation exposure in Ireland. Radiat Prot Dosim 128: 12-20.
- Won JL, Eun SC, Mina H, Young-Woo J, Seung-Sik H, et al. (2009) Occupational radiation doses among diagnostic radiation workers in South Korea. Radiat Prot Dosim 136: 50-55.
- (1990) Recommendations of the international commission on radiological protection. Ann ICRP 21: 1-3.
- (2002) Occupational radiation protection. Radiation protection and safety guide, GRPB-G3: 2000.
Author Details
HK Agyeman1*, BJB Nyarko1,2, S Shiloh1,2, F Adeku2, EO Darko1,2, JK Amoako1,2, J Owusu-Banahene1,2, S Inkoom1,2, DF Charles1, BD Bekoe1, O Adukpo1,2, G Tetteh1, DN Adjei1, BK Agyeman1, P Manteaw1, E Amoatey1, GO Aseidu1, J Gyasi1, P Appiah1, EM Abadoo1 and G Agyeman1
1Radiation Protection Institute, Ghana Atomic Energy Commission, Ghana
2Graduate School of Nuclear and Allied Sciences, University of Ghana, Atomic Campus, Kwabenya-Accra Ghana
Corresponding author
HK Agyeman, Radiation Protection Institute, Ghana Atomic Energy Commission, P O Box LG 80, Legon-Accra, Ghana.
Accepted: May 26, 2020 | Published Online: May 28, 2020
Citation: Agyeman HK, Nyarko BJB, Shiloh S, Adeku F, Darko EO, et al. (2020) Routine Care and Maintenance of Harshaw 6600 Plus (TLD) Reader in the Personnel Dosimetry Laboratory in Radiation Protection Institute in Ghana. Int J At Nucl Phys 5:019.
Copyright: © 2020 Agyeman HK, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Base on the routine care and maintenance of the Harshaw TLD 6600 Plus Reader, this publication will emphasize on the nominal value and tolerance parameters of the Harshaw TLD 6600 Plus Reader and the readout will be compared to the standard criteria, by analysing the records of quality control QC readouts and the co efficient of variation parameters respectively.
The parameters of the electronic QC which include the nominal value and tolerance parameters have been monitored and also compared to those of standard criteria. Moreover, the readout results which were obtained from the Personnel Dosimetry Laboratory show that the Harshaw TLD 6600 Plus Reader was working efficiently. Hence it can be used in the Personnel Dosimetry Laboratory.
This study serves as an integral component which contributes to the comprehensive routine measurements that are carried out daily in performing the electronic QC in the Personnel Dosimetry laboratory in Ghana Atomic Energy Commission.
Keywords
Quality control, Quality assurance, Calibration, Harshaw 6600 PLUS (TLD) reader, Ionizing radiation and exposure
Introduction
This publication gives a detailed activities carried out in the Personnel Dosimetry Laboratory during the year from January to December 2019, in the Health Physics and Instrumentation Centre of the Radiation Protection Centre in Ghana Atomic Energy Commission. The publication comment on the daily routine work, maintenance of the Harshaw TLD 6600 reader, commercial activities and some challenges face by the Personnel Dosimetry Laboratory. The Personnel Dosimetry Laboratory was set up to monitor all occupationally exposed workers, both nationally and internationally. The Personnel Dosimetry Laboratory assisted in training students, post graduates and under graduates and all the visitors that came to the Personnel Dosimetry Laboratory during their technical visits. Moreover, the Personnel Dosimeter Laboratory evaluated the doses from the TLD (Thermoluminiscent Dosimeter) by using the Dose Management System (DMS), provided by the International Atomic Energy Agency (IAEA)’s. This is a report that serves as a standard form of personnel monitoring service.
The Laboratory also updated the previous doses for every Occupationally Exposed Worker received since the commencement of Personal Monitoring Service.
Additionally, the Personnel Monitoring section of the Health Physics and Instrumentation Centre (HPIC), Radiation Protection Institute (RPI) engages in income generating services. The total number of people monitored was Six Hundred and Thirty-Two (632) which includes medical, radiotherapy, industrial and research facilities. The number of people for medical and radiotherapy facilities is Five Hundred and Fourteen (514), that of Industrial is Fifty-Eight (58) and Research is Sixty (60).
Earlier generations shows that, there have been various models of the Harshaw TLD Readers these include:
• Harshaw TLD 4500
• Harshaw TLD 3500
• Harshaw TLD 2000
• Instadose
Another evolution of the Harshaw TLD Reader has evolved out which is also known as Harshaw TLD 6600 Plus Reader.
The purpose and function of the Harshaw TLD reader are as follows:
• Measuring doses from whole body such as skin deep Hp (0.07) and Hp (10)
• Monitoring
• Neutron monitoring
Normally, different sources are installed in the Harshaw TLD reader but the radiation source which is commonly used in the Harshaw TLD 6600 Reader for calibration to convert the measuring signal to absorbed dose is 90Sr and the amount is 0.5 μCi respectively.
The model 6600 Plus have a serial number of 1808490 with an AC input and a voltage of 100, 120/220, 240 VAC, Frequency 50/60 Hz, Current 3.5/1.5 AMPS and VA 400.
The VAC TYPE:
• 100,120 3AG4ASLO
• 220,240 3AG2ASLO
Basically, before the Harshaw TLD 6600 reader can be used, it need to be loaded with TLD dosimeters and the loading capacity for the reader is 200 (TLD Dosimeters). The reader was used to measure the peak height and the integrated value of the glow curve. The type of TLD used was TLD TYPE: 0110, COLOR: COPPER with C.O. number; 198067 from thermo Fisher Scientific. Every TLD dosimeter has a different barcode attached to them. Some straps are also assigned to each TLD holder which is later assigned to the Occupational Expose Worker (Figure 1, Figure 2 and Figure 3).
Calibration of Harshaw (TLD) 6600 Plus Reader
The calibration of the Harshaw TLD 6600 Plus Reader helps establish the reader calibration factor (RCF). The RCF then helps to convert the output of the PMT in the Nano coulombs to the dosimeter unit respectively, for the temperature time profile (TTP) to be also established, the procedure must be repeated. Normally, when the temperature, time or rate field are subsequently changed for the preheat [1].
TLD are known to have energy dependence in kilo voltage region unlike in the megavoltage region where their response is relatively flat.
Calibrate Reader
The calibration of the Harshaw TLD 6600 Plus Reader is usually used to establish the Reader Calibration Factor (RCF) for Temperature, Time Profile (TTP), this is normally done for a newly defined TTP or as part of a regular quality assurance practice.
Basically, if the calibration is complete, the display of the nominal irradiation value from the screen is recorded. That is the nominal irradiation value to which the dosimeters were exposed. Additionally, there are other parameters that are also taken into consideration during the recording process such as:
• TTP Number
• The Group Number
• The Calibration Unit
The calibration unit is applied with the TTP when the RCF is applied.
Dosimeters which were out of range are normally removed and the dosimeters that fell within the range are usually used as acceptable for the calibration purposes.
Reports are then generated when the Technician, Technologist or the Research Scientist are satisfied with the statistics representing the calibration of the instrument. It is then sent to the Manager of the Laboratory for proof read to and to confirm the results. He later signs it if the results are okay.
Basically, after every three (3) months, for proper care and maintenance to be ensured, the Harshaw TLD 6600 Plus Reader must be recalibrated. The PMT must be replaced during this maintenance and services. Moreover, the high voltage power supply must also be adjusted.
Furthermore, TLD cards are usually picked randomly and used for the calibration purposes. These cards are annealed and exposed to a known amount of radiation. Later on, these cards are read with the reader cards function field set "Calibration Reader" and using the TTP to be calibrated.
A software known as WinREMS stores the raw data in the Group Database respectively.
Routine Quality Assurance
Reader Calibration Factor (RCF)
Normally, a new RCF is generated for all calibrated TTPs. This is usually done when the TTP is changed, the high voltage setting is changed and if the electronic QC is performed respectively.
Another option in performing the quality assurance procedure is that periodically checks the Reader calibration factor for commonly used TTP on a daily basis and record the RCF on a Daily Control Chart.
If the new RCF varies from the previous one either by one or 2%, you should seek a reason for a change.
Usually, the troubleshooting techniques in the Technical Reference Manual are used in the Section 6.4 Calibration Reader in the User manual for instructions on performing the calibration.
Terminology Defined
Temperature (℃): Normally, the temperature should be set at room temperature after a two hours (2 hr) cooling period.
High Voltage (volts): In general, the high voltage measures the voltage at each photomultiplier tube. It is normally adjustable but it should not be changed unnecessarily because it can affect all the Reader Calibration factors.
Plus 15 Volts: Basically, this voltage powers the analog electronics.
Minus 15 Volts: Is the voltage powering analog electronics.
D/A Reference: Moreover, D/A Reference is reference voltage of the digital-to-analog conversion circuit.
Reference Light: Refers to the equivalent TLD measurement of the constant light output from the built - in reference light source. The value should be consistent from day to day on any given channel.
PMT Noise: Is a reading of electronics noise generated by the photomultiplier tube, it should be also as low as possible but will never be zero in normal operation.
Sometimes, the number of PMT noise sample can be taken by the times of PMT background noise.
PMT: Photomutiplier Tube
TTP: Time Temperature Profile
TLD: Thermoluminescene Dosimeter.
Material and Methods
Material
For this project, the Harshaw TLD (Model 6600 Plus) located at the Radiation Protection Institute is the reader used for estimating whole body and extremity effective doses recorded by the TLDs. A non-contact heating system is used which utilizes a stream of hot nitrogen gas. The Reader is interfaced to a computer where all measured data can also be displayed, stored and printed. A hand held scanner is used to identify each TLD card before reading.
Thermoluminescent dosimeter: The most widely used material is the LiF with added magnesium and titanium. TLD-100 is LiF: Mg, Ti which consists of 92.5% of Li-7 and 7.5% of Li-6. Each card consists of four/two chips. In this project, five hundred (500) new two elements TLD 100 were used. The TLD cards are fixed in their holders which consist of two aluminium filters of different thicknesses; 0.07 mm (for skin dose measurements) and 10 mm (for deep dose measurements). One corner of the TLD card is notched to make sure it is placed correctly in the Reader holder system. The Reader holder system protects the cards from the environment and keeps the filtration media which attenuate different types of radiation in order to ensure selective entrapments of the TLD-100. Apart from the chips, each card has a unique barcode.
In this study, annual dose records of diagnostic radiology staff in the medical facilities for the period January - December 2019 were retrieved from the DMS and exported to Excel 2010 for analysis. The numbers of monitored exposed workers for each of the four previously mentioned categories are presented; as well as the dose distribution, annual collective dose and the mean annual dose.
The mean annual dose,
Where HT is the equivalent dose in tissue T and WT is the tissue weighting factor for tissue T
N = number of measurement in a year.
The annual collective dose, S, is given by
Where Eji is the annual dose calculated for the jth reading of the ith worker and N is the number of workers in a facility and r is the number of measurement in a year [2].
Results and Discussion
The graph show occupational radiation exposures of workers involved in ionizing radiation oriented practices in medical facilities. The minimum detectable limit is 0.1 mSv and the annual dose limit is 20 mSv averaged over five years.
Figure 4 indicates the distribution of annual personal dose records from 2011 to 2015; about 51% were below 1 mSv and 49% between 1 mSv and 5 mSv.
Table 1 indicates the annual average effective dose of all the occupationally exposed workers falls in the range of 0.36-1.70 mSv. The highest annual average effective dose 1.70 mSv was found in Radiographers category in the year 2015. This could be due to the increased number and operations of x-ray radiography facilities.
In Table 2 which shows the annual collective dose and their percentage contribution, averaged over the five (5) year period for the various category of workers. General radiography recorded the highest collective dose followed by CT technology, radiology, and fluoroscopy technology which are 21.87 person Sv (89.14%), 1.58 person Sv (5.98%), 0.85 person Sv (3.73%) and 0.27 person Sv (1.16%) respectively. The range of annual total collective effective dose was found to be 0.1- 42.48 person Sv.
Individual dose records for one thousand five hundred and seventy-four (1,574) OEWs from diagnostic radiology facilities were analyzed in this study during the 5 year period (2011-2019) and findings presented in Table 1 and Table 2. The percentage distribution is as follows: General radiographers (63%), radiologists (13%), CT technologists (17%) and fluoroscopy technologists (7%), who were all measurably exposed. The highest annual individual dose recorded was 8.48 mSv received by an interventional radiologist in 2015 and the least being 1.27 mSv for a CT technologist in 2012. During routine work, CT technologists are normally inside the control booth and are shielded from scatter radiation from the patient. The low annual individual dose demonstrates the adequacy of structural shielding in these facilities.
The monitored medical facilities increased by 31.25%, while the exposed workers increased by 55.83% over the study period [3]. This is attributed to the sharp rise in the number of diagnostic radiology facilities licensed or authorized by the Radiation Protection Board over the period.
For all the workers monitored, the doses observed over the 5-year period were well below the internationally recommended limit of 20 mSv per year and this is due to the fact that the workers were sensitized on the essence of personal monitoring and radiation principle of optimization. This led to improvement in some of their radiation protection practices in the course of their work.
Conclusion
The average annual effective doses of occupational radiation exposure among diagnostic workers decreased substantially during the study period. This could be due to improvement in radiation protection protocols in the respective facilities. Exposed workers in the conventional X-ray facilities received the highest individual doses. Correspondingly their collective dose represented 96% of the total collective dose during the period. Average doses per the medical institution and exposed workers were 5 and 0.73 mSv, respectively in the entire survey period. This study provided an opportunity to understand the trends in the occupational radiation doses and the working environment and will form the basis for a national database of exposures for radiation workers that can be used to assess potential adverse radiation effect [4].
Parameters Defined
Temperature: Normally, the temperature should be set at room temperature after a two hours (2 hr) cooling period.
High Voltage: In general, the high voltage measures the voltage at each photomultiplier tube. It is normally adjustable but it should not be changed unnecessarily because it can affect all the Reader Calibration factors.
Plus 15 Volts: Basically, this voltage powers the analog electronics.
Minus 15 Volts: Is the voltage powering analog electronics.
D/A Reference: Moreover, D/A Reference is reference voltage of the digital-to-analog conversion circuit.
Reference Light: Refers to the equivalent TLD measurement of the constant light output from the built-in reference light source. The value should be consistence from day to day on any given channel.
PMT Noise: Is a reading of electronics noise generated by the photomultiplier tube, it should be also as low as possible but will never be zero in normal operation.
Sometimes, the number of PMT noise sample can be taken by the times of PMT background noise.
PMT: Photomultiplier tube.
TTP: Time Temperature Profile.
TLD: Thermoluminescence Dosimeter (Table 3).
Routine Quality Assurance
Reader Calibration Factor (RCF)
Normally, a new RCF is generated for all calibrated TTPs. This is usually done when the TTP is changed, the high voltage setting is changed and if the electronic QC is performed respectively.
Another option in performing the quality assurance procedure is that periodically checks the Reader calibration factor for commonly used TTP on a daily basis and record the RCF on a Daily Control Chart.
If the new RCF varies from the previous one either by one or 2%, you should seek a reason for a change.
Usually, the troubleshooting techniques in the Technical Reference Manual are used in the Section 6.4 Calibration Reader in the User manual for instructions on performing the calibration [5].