International Journal of Biomechanics and Movement Science
(ISSN: 2631-5114)
Volume 4, Issue 1
Research Article
DOI: 10.35840/2633-8955/9725

Article Formats
Conservative and Surgical Treatment of Lumbar Disc Herniation
Table of Content
Figures
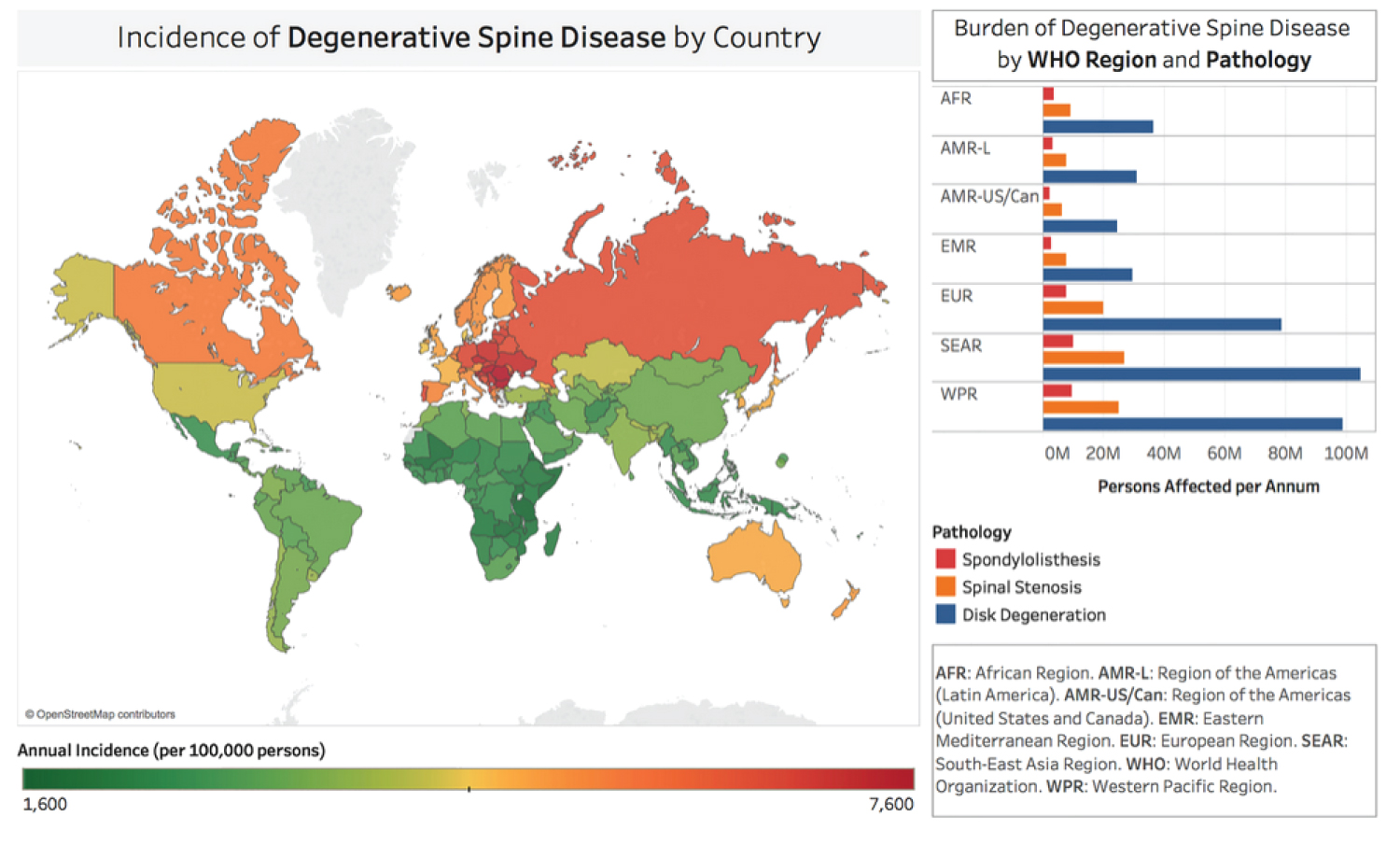
Figure 1: Incidence rates of degenerative...
Incidence rates of degenerative spine disease/low back pain in World Bank and World Health Organization recognized countries (2023). Fonte: journals.sagepub.com/doi/10.1177/2192568218770769.
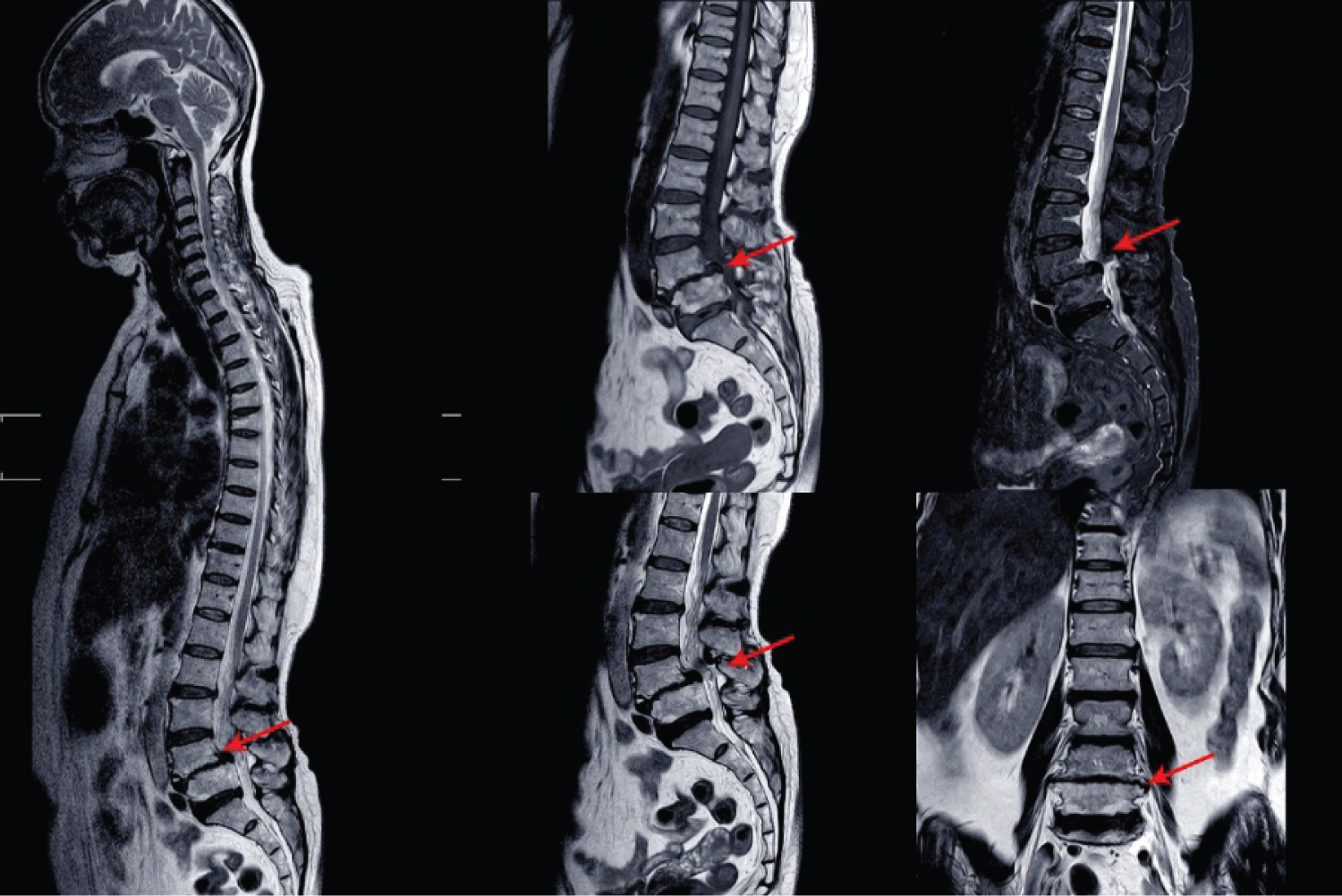
Figure 2: Lumbar lesion shown on MRI....
Lumbar lesion shown on MRI of the lumbar region. Source: therafit.com/Injuries-Conditions/Lower-Back/Lower-Back-Issues/Low-Back-Pain/a~1452/article.html
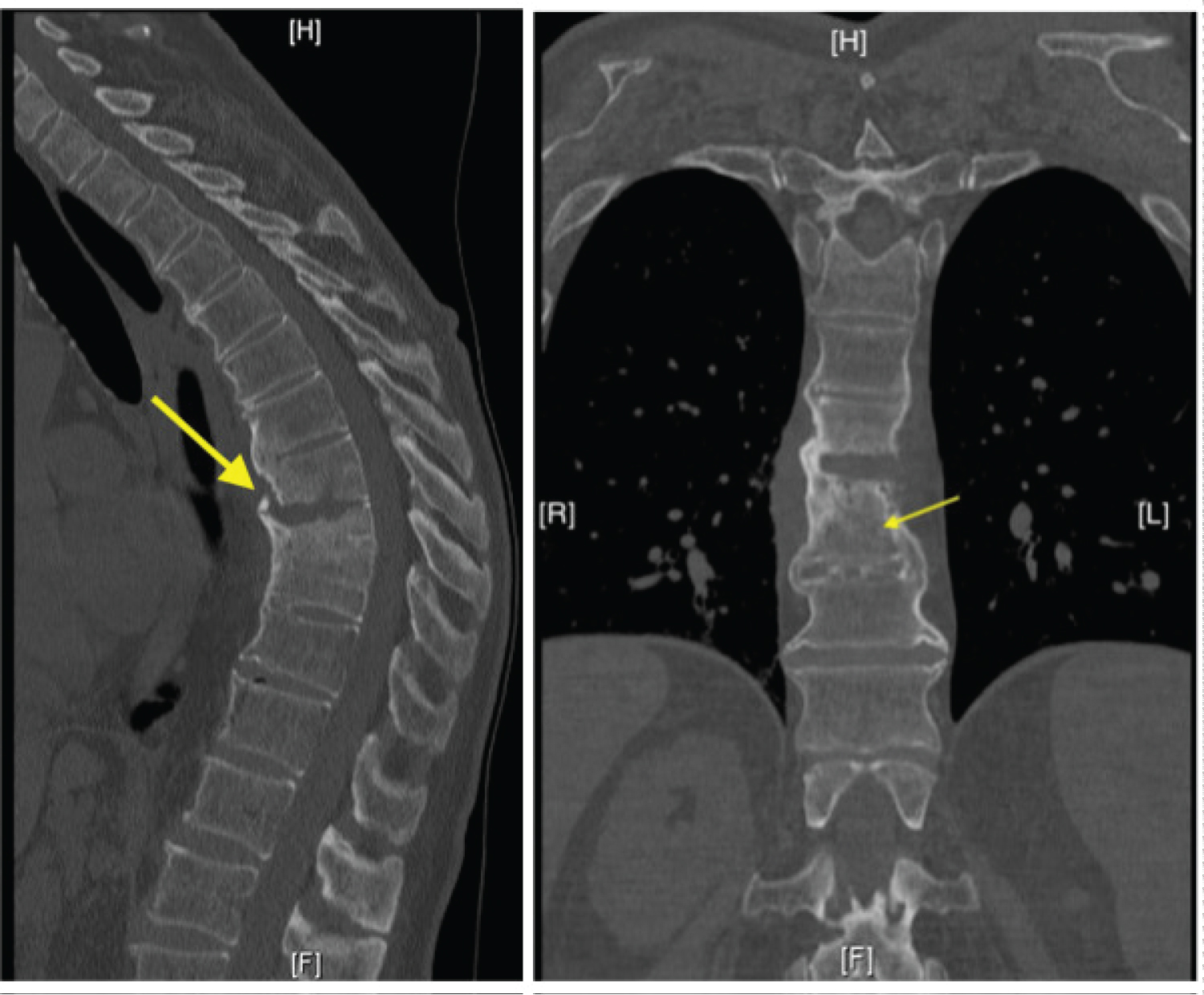
Figure 3: CT scan of the spine with....
CT scan of the spine with suspicious findings of discitis/osteomyelitis at T8-9 (arrow). Source: orthopedicreviews.openmedicalpublishing.org/article/32243-an-ominous-cause-of-back-painvertebral-osteomyelitis

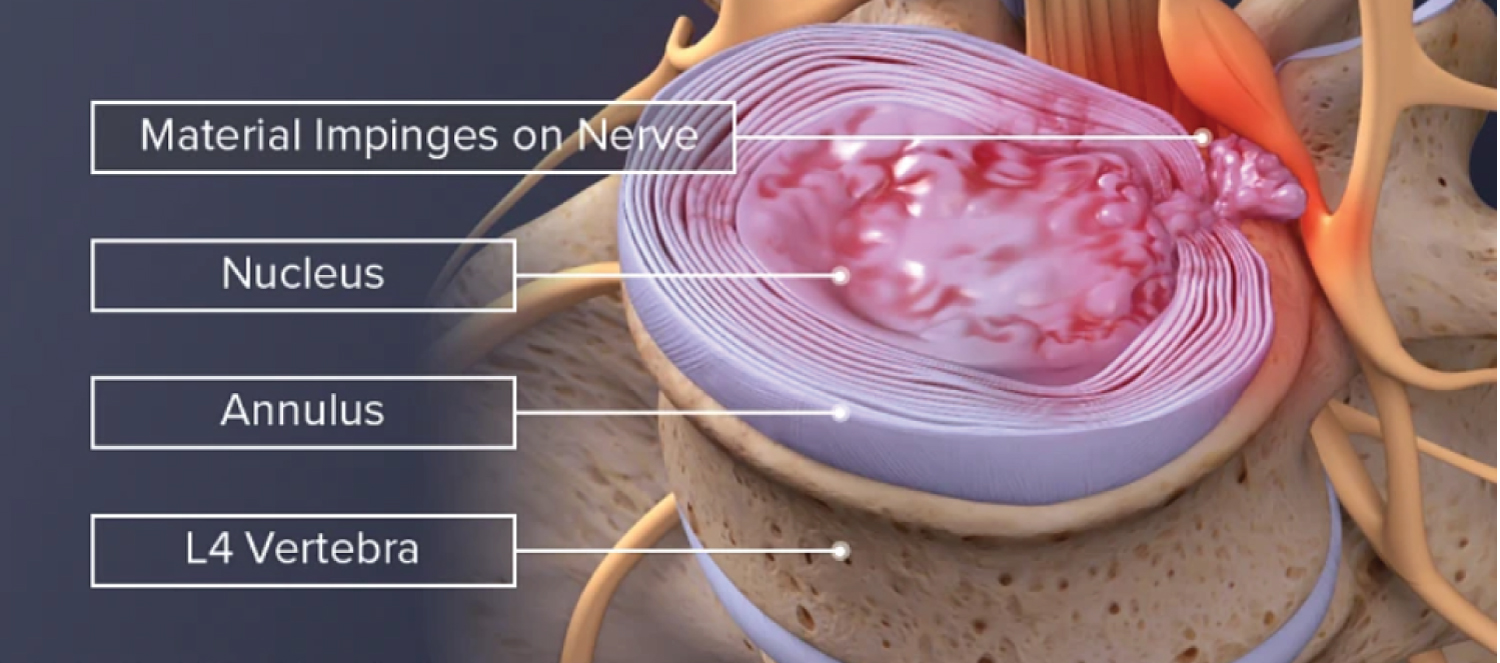
Figure 5: Various degrees of disc....
Various degrees of disc herniation can be treated with microdiscectomy.
Source: spine-health.com/treatment/back-surgery/microdiscectomy-microdecompression-spine-surgery.
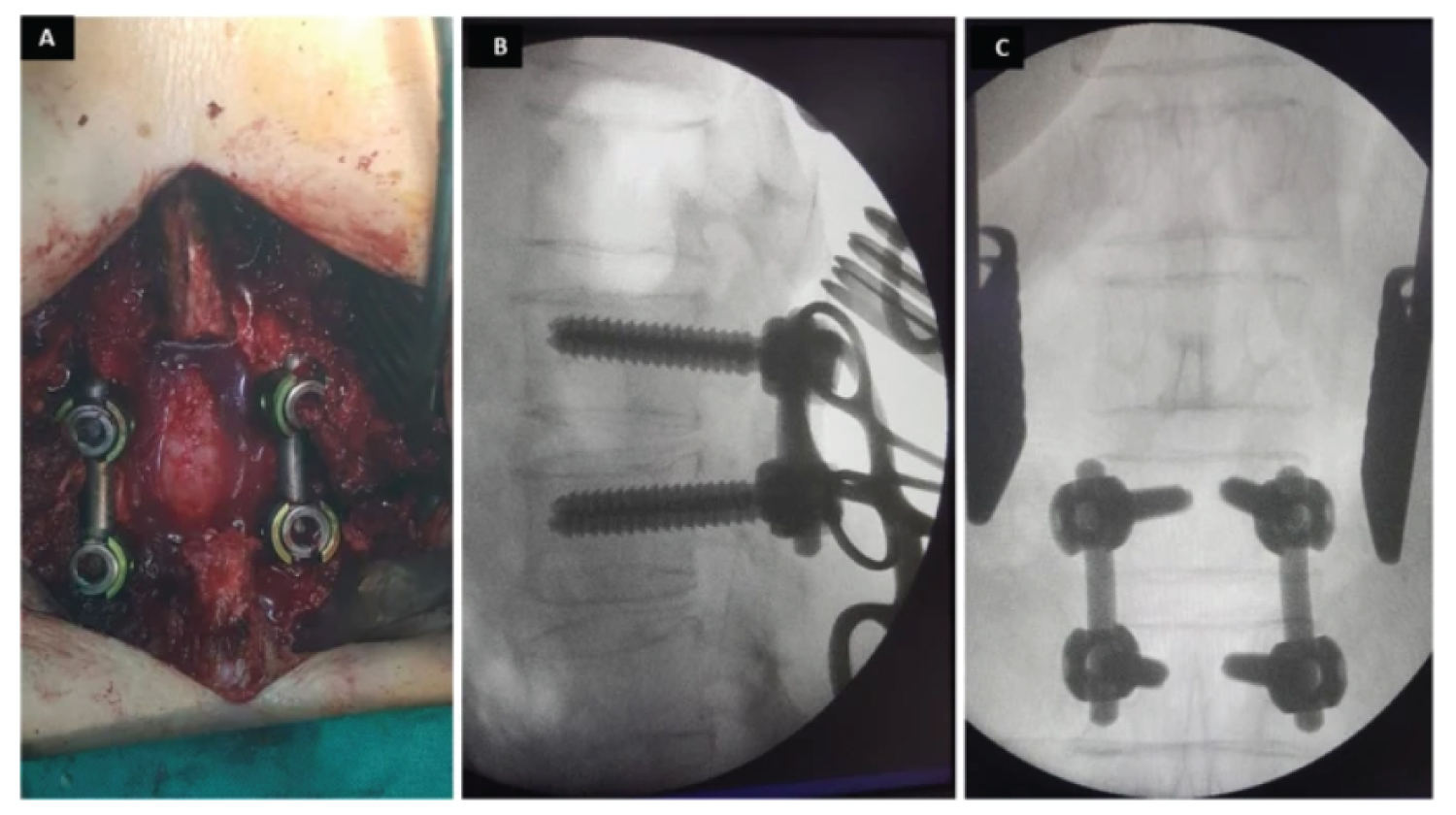
Figure 6: Intraoperative view of the....
Intraoperative view of the same patient (a) showing the extent of the laminectomy and the final fixation of the transpedicular screw. Intraoperative fluoroscopic images b lateral view and c AP view showing the exact placement of the pedicle screw fixation at L1-L2.
References
- Sergio H, De Abreu MR (2020) Estenose degenerativa do canal lombar. Revista Brasileira de Ortopedia 56: 9-17.
- Guida CA, Ferreira VJ, De Souza FV (2020) Percepção do portador de hérnia de disco acerca do tratamento fisioterapêutico. Bionorte 9: 26-35.
- Denis S (2021) O efeito da terapia manual no alívio da dor em indivíduos com disfunção sacroilíaca: Uma revisão sistemática. Seminário Nacional de Pesquisa.
- Augusto FG (2022) Existe correlação entre grau de degeneração discal e lombalgia? Tese de Doutorado. [sn].
- Gomes MH, de Queiroz JGV, Souza RBE, Bernardes CI, da Silva Jessica Aguilar et al. (2023) Tratamento de dor radicular da hérnia de disco lombar: Microdiscectomia versus abordagens fisioterapêuticas. Revista Eletrônica Acervo Saúde 23: e14392-e14392.
- Castro AFA, Furtado GAL, de Melo BA (2021) Conservative versus surgical treatment in patients with lumbar disc herniation. BrJP 4: 357-361.
- Dos Santos PS, de Oliveira SJ, de Oliveira JP, Torres CA (2021) Estudo clínico randomizado no tratamento da hérnia de disco lombar. Revista Saúde e Desenvolvimento 15: 93-106.
- Mendes FL (2024) Entrevista com Médico Ortopedista a respeito das dores lombares.
- van den Hout WB, Peul WC, Koes BW, Brand R, Kievit J, et al. (2008) Prolonged conservative care versus early surgery in patients with sciatica from lumbar disc herniation: Cost utility analysis alongside a randomised controlled trial. BMJ 336: 1351-1354.
- Huang R, Meng Z, Cao Y, Yu J, Wang S, et al. (2019) Nonsurgical medical treatment in the management of pain due to lumbar disc prolapse: A network meta-analysis. Semin Arthritis Rheum 49: 303-313.
- Tiendrebeogo/Zabsonre WJS, Zabsonre DS, Kabore F, Sanou A, Haro Y, et al. (2024) Pediatrics severe low back pain by disc herniation: An uncommon entity. Pediatr Rheumatol Online J 22: 1.
- Wardlaw D (2016) Sciatica caused by disc herniation: Why is Chymopapain Chemonucleolysis denied to our patients? Int J Spine Surg 10: 44.
- Asgharzadeh A, Khoshnood N (2017) Evaluating the safety and efficacy of discogel in the treatment of herniated lumbar disc: A systematic review. Health Technology Assessment in Action
- Lefe`vre-Colau M-M, Babinet A, Poiraudeau S (2024) Traitement des lomboradiculalgies. EMC-Rhumatologie-Orthopédie 1: 328-342.
- Homotetski D (2014) Effectivness of conservative and microdiscetomy treatment for patients with lumbar disc herniation.
- Alexandre A, Corò L, Paradiso R, Dall'aglio R, Alexandre AM, et al. (2011) Treatment of symptomatic lumbar spinal degenerative pathologies by means of combined conservative biochemical treatments. Acta Neurochir Suppl 108: 127-135.
- Lühmann D, Burkhardt-Hammer T, Borowski C, Raspe H (2005) Minimally invasive surgical procedures for the treatment of lumbar disc herniation. GMS Health Technol Assess 1: Doc07.
- Valls I, Saraux A, Goupille P, Khoreichi A, Baron D, et al. (2023) Factors predicting radical treatment after in-hospital conservative management of disk-related sciatica. Joint Bone Spine 68: 50-58.
- Reiman MP, Sylvain J, Loudon JK, Goode A (2015) Return to sport after open and microdiscectomy surgery versus conservative treatment for lumbar disc herniation: A systematic review with meta-analysis. Br J Sports Med 50: 221-230.
- Shahbandar L, Press J (2021) Diagnosis and nonoperative management of lumbar disk herniation. Operative Techniques in Sports Medicine 13: 114-121.
- Wilby MJ, Best A, Wood E, Burnside G, Bedson E, et al. (2021) Surgical microdiscectomy versus transforaminal epidural steroid injection in patients with sciatica secondary to herniated lumbar disc (NERVES): A phase 3, multicentre, open-label, randomised controlled trial and economic evaluation. Lancet Rheumatol 3: e347-e356.
- Codignole A, Faria MD, Oliveira AA, Cobos LD, dos Santos ECF, et al. (2021) Síndrome da cauda equina causada por compressão de hérnia de disco lombaR. RECIMA21-Revista Científica Multidisciplinar 2: e28626-e28626.
Author Details
Guilherme I Santos1, Thalita PM Alineri1, Délio TM Malaquias1, Juliana Paschoal1, Isabeli G Oliveira1, Brenda MMR Oliveira1, Eliza F Prezotto1, Isadora O Soler1, Bruna D Araujo1, Caroline P Golin1, Maria Gabriela S Guzzi1, Igor F Forechi1, Guilherme G Martins1, Ana Clara F Parreira1, Cindy Vilarinho1, Samantha RG Sanches1
11Academic in Medicine, University of Ribeirão Preto, Campus Guarujá, São Paulo, Brazil
2Academic in Medicine, University Potiguar, Natal, Rio Grande do Norte, Brazil
3Academic in Medicine, University of Southern Santa Catarina (Unisul), Tubarão, SC, Brazil
4Medical Student, Nove de Julho University, São Bernardo do Campo, São Paulo, Brazil
5Bachelor of Medicine, Nove de Julho University, São Bernardo do Campo, São Paulo, Brazil
6MSc and PhD in Orthopaedics, Traumatology and Rehabilitation of the Locomotor System, Bachelor's degree in Physical Education, Ribeirão Preto Medical School, Federal University of São Carlos, University of São Paulo, Brazil
7Medical Residency in Orthopaedics and Traumatology at Irmandade Santa Casa de Santos-SP, Specialization in Orthopaedics and Traumatology in the area of shoulder and elbow, Postgraduate Latu Sensu in Chronic Pain Intervention, Member of the Brazilian Orthopaedic Society, Bachelor of Medicine, Federal University of Minas Gerais, Belo Horizonte-MG, Brazil
Corresponding author
Thiago AR Bezerra, Academic in Medicine, University of Ribeirão Preto, Campus Guarujá, São Paulo, Brazil; MSc and PhD in Orthopaedics, Traumatology and Rehabilitation of the Locomotor System, Bachelor's degree in Physical Education, Ribeirão Preto Medical School, Federal University of São Carlos, University of São Paulo, Brazil.
Accepted: March 16, 2024 | Published Online: March 18, 2024
Citation: Santos GI, Alineri TPM, Malaquias DTM, Paschoal J, Oliveira IG, et al. (2024) Conservative and Surgical Treatment of Lumbar Disc Herniation. Int J Biomech Mov Sci 4:005
Copyright: © 2024 Santos GI, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: A herniated disc occurs when the disc that acts as a cushion between the vertebrae of the spine shifts and presses on nearby nerves. The L4-L5 region refers to the lumbar vertebrae located in the lower back. A herniated disc in this region can cause pain, tingling, muscle weakness and even the inability to perform daily tasks. Evidence comparing the effectiveness of surgical and conservative treatment for symptomatic lumbar disc herniation is controversial.
Objectives: The aim of this study is to discuss, through a literature review, the pros and cons of conservative and surgical treatment for herniated discs, as well as their risks and benefits according to current medical advances.
Results and discussion: Compared to conservative therapy, surgical treatment provided faster relief of low back pain symptoms in patients with lumbar disc herniation, but showed no benefits over conservative treatment in medium and long-term follow-up.
Final considerations: Surgical treatment may therefore be attractive for patients with debilitating pain symptoms who are looking for rapid relief or who have not achieved satisfactory improvement with conservative treatment.
Keywords
Surgery, Conservative, Hernia, Prolapse, Sciatica
Introduction
Low back pain is one of the most frequent complaints in the doctor's office. Among the causes of low back pain we can find;
One of the main causes of pain is myofacial pain. According to Hennemann, et al. [1], myofascial pain is perceived by the stimulus, such as muscle stiffness that is generated in the trigger points of the muscles. Factors that intensify the risk of trigger points are muscle injuries, repetitive movements, poor posture, stress and anxiety.
Another complaint is joint pain between the interapophyseal joints. This pain usually leads to limited mobility. Interapophyseal arthrosis can reduce the range of movement of the spine, making movements more restricted. Pain worsens with activity, and pain in the interapophyseal joints tends to worsen with physical activity or after sitting or standing for long periods [2].
According to Smith, et al. [3], another issue to be pointed out is pain in the sacroiliac joint. Sacroiliitis is the term used for inflammation in one or both sacroiliac joints, the site of communication between the spine and the pelvis. The problem can occur for different reasons and is typically accompanied by lower back pain and stiffness, pain in the buttocks and, eventually, pain radiating to the lower limbs.
One cannot fail to mention pain of disc origin (discogenic). According to Foizer [4], discogenic pain occurs when there is degeneration of the intervertebral disc. This disc is located between the vertebrae of the spine and acts as a shock absorber, distributing loads and allowing mobility.
Another issue is radicular pain caused by nerve compression due to a herniated disc. Radicular syndrome is often caused by direct pressure from a herniated disc or degenerative changes in the spine that cause irritation and inflammation of the nerve roots by bone spurs popularly known as "parrot's beaks" or collapse of the nerve root tunnels (foramen) [5].
These conditions can cause severe pain, functional limitations and affect the ability to perform everyday tasks, including work. The disability caused by spinal problems can range from moderate discomfort to severe difficulties that completely prevent the performance of professional activities.
According to data collected from the Brazilian Ministry of Social Security, in 2021 alone, 51,400 beneficiaries had to leave work to undergo treatment for herniated discs. A sedentary lifestyle and poor posture are identified by medical specialists as the main factors associated with back problems [6].
According to Guida, et al. [2], herniated discs occur mainly between the fourth and fifth decades of life (average age 37 years), although they have been described in all age groups. It is estimated that 2 to 3% of the population may be affected, with a prevalence of 4.8% in men and 2.5% in women over the age of 35.
Herniated discs affect around 5.4 million Brazilians. According to the WHO (World Health Organization), eight out of ten people in the world suffer from herniated discs, a condition that is one of the main causes of low back pain [7].
The term lumbago refers to low back pain. The term lumbago refers to low back pain. ciatalgia is pain due to nerve compression of the sciatic nerve, which in this case is pain that radiates down the back of the thigh, crossing the knee, and lumbosciatalgia is a mixture of the two [8].
When we talk about pain, there are different types of pain. This includes pain in general, not just lower back pain [8].
According to orthopedic surgeon Leonardo Mendes Faria [8], examples of pain include nosciceptive pain: pain of traumatic or inflammatory origin; when there is a bruise or tendonitis; neuropathic pain: due to compression of a nerve. In this case we have neurological deficits, loss of strength or sensory symptoms (numbness, tingling, burning). To describe these symptoms we use the term paresthesia); mixed pain: comprises a mixture of these causes.
With these concepts in mind, when we describe the symptoms of low back pain due to a herniated disc. We will talk about pain in the lumbar region with irradiation to the gluteal region and posterior thigh that crosses the knee. This radiating pain may or may not be accompanied by neurological symptoms, such as loss of muscle strength or paresthesia. These symptoms will depend on the location of the hernia, i.e. which nerve root is being compressed [8].
Other symptoms include: Spinal rigidity, disappearance of the normal lordotic curve, muscle spasms, paresthesia, decreased or absent reflexes and sensory loss (with weakness in the myotome supplied by the compressed root) [9].
Lateral, foraminal and distant lateral hernias are usually more common than central hernias.
In vertebral discs, what happens is that the outermost region, which is more fibrous, breaks down over time, and so the gelatinous nucleus is "expelled", which can compress a nerve root on its own or the spinal cord itself [10].
According to Huang, et al. [10], low back pain can be classified in different ways, according to parameters such as time, cause and etiology;
A) Primary and secondary
We can classify the causes of low back pain as primary and secondary.''The primary ones occur if some local factor involving the structure of the spine leads to the pain; the secondary ones are when factors at a distance or not specific to the spine are responsible for the pain'' [10].
B) Acute and chronic
Acute pain (with less than 4 weeks of evolution) is observed in situations such as stretches, muscle contractures and herniated discs, which are the most frequent causes of low back pain [10]. Chronic pain (more than 12 weeks of evolution) is observed in other conditions, such as stenosis of the lumbar canal [11].
The aim of this paper is to discuss, through a literature review, the pros and cons of conservative and surgical treatment for herniated discs, as well as their risks and benefits according to current medical advances.
Methodology
This is a retrospective and prospective observational study in which the most common symptoms related to the locomotor system were considered: Low Back Pain, Lumbar Disc Herniation.
A search strategy was developed based on the evaluation of an objective on the subject in question, which forms the basis of the study. These were: Surgical and conservative treatment of lumbosciatalgia due to disc herniation, conservative and surgical processes.
The search descriptors were selected from the Descriptors in Health Sciences (DeCS) website and then combined with the Boolean operator "AND".
The databases used for the search were PubMed and the Virtual Health Library (VHL), which evaluated cross-sectional, cohort and case-control studies in Portuguese, English and Spanish.
The inclusion criteria were cross-sectional studies which were freely available and focused on the surgical and conservative treatment of lumbosciatalgia due to herniated discs.
In all, the result of the search in the databases using the descriptors, but without the application of filters, resulted in 53 available articles. After applying the following filters: PubMed: Portuguese, English and Spanish language and type of literature being a cross-sectional study. BVS: Portuguese, English and Spanish language and type of literature being an observational study, a total of 26 articles were selected.
Results and Discussion
The results of the findings are presented in several topics, aiming to provide knowledge about the process that leads to low back pain, including forms of treatment.
Low back pain and diagnosis
Low back pain is pain that affects the lumbar region, the lower part of the back below the ribs. This is an area of the spine made up of 5 vertebrae and the sacrum, establishing a connection between the upper and lower body and supporting most of our weight. Due to these functions, the sacrum is easily prone to injury when subjected to sudden movements such as lifting, twisting, etc [11].
In common mechanical low back pain (the most prevalent form), most cases are limited to the lumbar region and buttocks, rarely radiating to the thighs. The pain may appear suddenly in the morning and be accompanied by antalgic scoliosis. The episode lasts an average of 3 to 4 days and, after this time, the patient returns to normal with or without treatment [12].
Low back pain can be a symptom of various pathologies affecting the spine, including degenerative, inflammatory, infectious, neoplastic, metabolic, dermatological and traumatic diseases [10].
Herniated discs can also be a symptom of radiating pain (related to problems in peripheral joints, such as the hip joint) or even referred pain, coming from a pathology in internal organs. This extensive differential diagnosis makes the initial assessment of low back pain a challenge. The patient is often subjected to various (expensive and unnecessary) laboratory and imaging investigations. It is therefore important to have an algorithm for clinical reasoning that facilitates initial management, diagnosis and the prevention of complications in the most serious cases [12].
First of all, the anamnesis is extremely important. Although the physical examination provides a lot of information, such as limitation of movement, deformities, myofascial pain points and neurological involvement, in most cases it alone does not allow for a certain diagnosis [12].
Laboratory tests are generally normal and should only be requested under specific conditions [12].
The main factor in misdiagnosis when assessing low back pain is the overvaluation of imaging tests. This is because the spine changes its shape with little or no relation to the presence of symptoms, both in simple X-ray (XR) alterations and in computed tomography (CT) or magnetic resonance imaging (MRI). Thus, both imaging and other complementary tests are used in cases of patients with suspected neurological damage or specific low back pain [13].
Figure 1 shows the degenerative incidence of the spine in a global perspective according to data from the World Health Organization in the year 2023.
Origin of low back pain
Low back pain can originate from the muscles that support the lumbar spine, from the interspinous ligaments between the vertebrae, from the joint apophyses that may be inflamed, from the sacroiliac joints - close to the hip, from the vertebral discs that are not properly cushioning the impact on the spine or from mechanical or chemical irritation of the dura mater [11].
Low back pain of mechanical etiology
Low back pain of mechanical etiology is caused by congenital anomalies, where the spine is incorrectly formed. For example spina bifida (vertebral spinous process is "split") or sacralization/lumbarization of a vertebra; also degenerative causes, in which the patient gradually loses function and/or wears out. Examples include: Spondylarthrosis and spondylolysis; discogenic syndromes (Figure 2), where disc prolapse can cause pain; and trauma, due to various causes such as falls, weight bearing, accidents, etc [10].
Low back pain of inflammatory etiology
The inflammatory etiology of low back pain is caused by systemic diseases that generate inflammation [14].
For Lühmann, et al. [15], a common cause is ankylosing spondylitis, which causes fusion of the vertebrae and inflammation, thus causing pain.
Another cause is rheumatoid arthritis, which wears down the joints and thus generates low back pain; there is fibromyalgia, which causes chronic pain in different parts of the body [10].
Low back pain of infectious etiology
These are the smallest causes of low back pain (0.01%), and there is always an associated fever. It can affect patients who use intravenous drugs or who have had recent infections [16].
It is closely associated with staphylococci, the most common microorganism in these cases [12].
It can also be due to Pott's disease, which is bone tuberculosis (TB) when it affects the lumbar spine (investigate if there has been contact with people infected with TB or a history of TB). Figure 3 shows a Computed Tomography (CT) scan of the spine with suspicious findings of discitis/osteomyelitis at T8-9 (arrow).
Low back pain of metabolic etiology
Osteoporosis can be mentioned, which although it doesn't hurt, can alter the alignment of the spine, fracture vertebrae, etc., leading to pain; there is osteomalacia, which is the softening of the bone, which can also lead to fractures and pain; hyperparathyroidism also comes into play here, because with the increase in PTH the calcium in the bones is consumed more and this leads to weakening, which also leads to fractures and pain [16].
Low back pain of tumor etiology
Various tumors can affect the spine, causing the patient (usually > 50-years-old) to lose weight, suffer nocturnal pain that causes them to wake up because of it, and feel tired [10]. Figure 4 shows a tumor at C4.
According to Lühmann, et al. [15], tumors can be intradural or extradural, compressing the disc and nerves or even causing bone damage and fractures, which is why myalgia occurs.
The lumbar can be affected by both benign and malignant tumors. If the pain is more localized, it tends to be benign; if it is more diffuse, sometimes together with systemic manifestations, it tends to be a malignant tumor. In general, benign tumors involve the posterior arch of the vertebra, while malignant tumors initially involve the vertebral body [11].
The most common benign tumor of the spine is hemangioma, while the most common malignant tumor is multiple myeloma (we can also see metastases coming mainly from the breast, lung, prostate, kidney, thyroid, bladder and colon) [9].
In malignant tumors, low back pain is the initial symptom in around 35% of cases. As mentioned, most episodes of low back pain evolve in a limited way, but around 10% (chronic pain) are responsible for the majority of cases of disability and most of the costs of low back pain. There are several risk factors that directly and indirectly increase an individual's risk of developing recurrent low back pain [17].
Obesity is one of the most studied factors, with several related mechanisms such as: Mechanical overload of the lumbar spine, association with chronic systemic inflammation, degenerative discopathy and changes in the vertebral plate. Another factor is smoking, especially in younger people. Genetic influence has also been studied extensively, showing a high risk of developing low back pain in twins if the pair has the pain. Other associated risk factors are: Psychological aspects (hysteria, neurosis; conversion disorders and depression) and level of education (people with fewer years of education are more likely to develop low back pain); as well as services that involve lifting loads [9].
While biomechanical causes are more associated with acute low back pain, the risk of chronification is more associated with factors such as fear, avoidance, catastrophism, depression, work situation, etc [16].
General treatment of low back pain
When it comes to treatment, it can basically be summed up as two types of treatment: conservative and surgical.
Conservative treatment already includes pharmacological treatment and rehabilitation (physiotherapy, core strengthening, etc.).
Surgical treatment - it's very important to talk about the criteria for surgical indication, such as;
✓ Installed neurological deficit, in this case loss of strength in a myotome.
✓ Signs of cauda equina.
✓ Sciatic pain without improvement in the first 6 weeks of conservative treatment.
Low back pain can be treated pharmacologically, non-pharmacologically or surgically, depending on the case [11].
For treatment, some non-pharmacological measures can be adopted to try to relieve the pain, such as thermotherapy (heat), spinal manipulation (through physiotherapy) and, finally, pharmacological therapy [9].
Sub-acute and chronic low back pain
In these cases, as a non-pharmacological measure, physical exercise can help in various aspects, from joint range to flexibility, recovery of muscle potential, adaptation to effort and so on. You can also use equipment such as laser, ultrasound, TENS, etc. Finally, other measures include massage, cognitive-behavioral therapy and acupuncture. In more severe cases, pharmacological therapy and even surgery are used [11].
Non-pharmacological therapy for low back pain
This is based on behavioral changes such as weight loss, physical exercise, physiotherapy and therapeutic measures such as cognitive-behavioral therapy, acupuncture, etc. Rest should be discouraged and guidance given to maintaining routine activities, as this leads to faster recovery and less disability in the long term [9].
Pharmacological therapy for low back pain
Valls, et al. [16], in their studies of this or that around 90% of low back pain improves spontaneously within a period of 30 days. However, it is common to prescribe medication such as non-steroidal anti-inflammatory drugs.
According to Reiman, et al. [18], symptomatic treatment should follow the pain scale, in a graded manner. Thus, it is important to weigh up the possible side effects, analyzing the risk-benefit ratio. In addition, treatment should be directed at the etiology, so infectious causes should be treated with antibiotics, inflammatory causes with corticosteroids and systemic causes according to their recommendations. Antidepressants, usually tricyclics, are among the most commonly used drugs in the treatment of chronic non-specific low back pain, whether or not associated with depression.
Conservative vs. surgical treatment of low back pain
The role of treatment in low back pain is mostly conservative (non-surgical), since the vast majority of patients improve before any more aggressive therapy is considered [16].
According to Homotetsky [19], the aim of treatment is to re-establish the balance of the spine, which has been compromised by the herniated disc. Only a small number of patients require surgery, and the majority are able to resolve the condition with conservative treatment alone.
According to Shahbandar, et al. [20], conservative treatment is a safe method, especially since the horizontal position relieves radiating pain in many patients. However, the rest period should only be for the reduction of the inflammatory process, and the return to activities should occur gradually, one week after the start of rest.
Surgery occurs when the natural course of the pathology worsens significantly after the use of non-aggressive measures. According to Tiendrebeogo [11], surgery is indicated because it depends on the duration of the symptoms, the stenosis of the spinal canal and the quality and severity of the symptoms.
However, Van Den Hout, et al. [9] pointed out that the procedure exposes the spine and removes the damaged disc. It brings faster improvement, but it is an invasive procedure that carries risks, and conservative treatment is preferred by most doctors and patients.
Several studies have investigated the preference for conservative care versus surgical decompression for sciatica from a herniated disc [16].
In the studies by Alexandre, et al. [14], 91% of patients achieved results with conservative measures. Around 80% of patients improve with conservative care over many months. However, one of the problems with lumbar disc herniation is that many sufferers are between the ages of 40 and 45, so there is a loss of livelihood if it is not managed quickly.
Even with just observation (literally doing nothing), some herniated discs can reabsorb on their own, like a bruise disappearing into your arm or leg. Most sequestered discs (a piece of the disc, free fragment, has been completely severed from the main disc) completely resolve after 9 months, while extruded discs (piece of the disc mostly, but the inner core still attached) disappear completely after 12 months. Disc herniations trigger an inflammatory response in which immune cells degrade the disc fragment [11].
For Lühmann, et al. [15], injecting medications such as chymopapain into herniated discs can physically degrade the disc (chemonucleolysis) and patients improve for a while. However, they often develop worse disc disease later on, probably secondary to the effect of chymopapain on the normal disc as well. This is why esmonucleolysis has lost its place as a form of treatment.
Spinal injections, including epidural steroid injections, have been used for a while [14].
According to Shahbandar, et al. [20], some of the controversy with spinal injections lies in the possible placebo aspect. Some studies have shown (including a major article in the New England Journal of Medicine in 2014) that lidocaine injections are no better than steroids alone, calling into question what an injection does in the setting of disc herniation.
Traditionally it was thought that patients have symptoms mainly of inflammation induced by compression on the nerve. After all, the mere presence of a herniated disc means nothing, even completely asymptomatic people have herniated discs [11].
However, the release of inflammatory factors, an immune response mediated by cytokines, causes the pain. That some patients release inflammatory markers that cause symptoms, and others do not, may not be fully understood [16].
According to Shahbandar, et al. [20], surgery is very effective. Surgery and time are the only two legitimate options for physically separating a disc fragment from the nerve.
A 2016 article in the British Medical Journal indicated that surgery has been shown to provide faster relief of lumbar disc herniation symptoms compared to conservative approaches [16].
A 2020 study evaluating 790 patients showed that when sciatica lasts more than 4 months, surgery was superior in relation to pain intensity at 6 months. However, there are also risks to surgery [16].
A study by Nerves, et al. [21] in the Lancet was published as a multicenter randomized controlled trial. Participants were randomly assigned to transforaminal epidural steroid injection or surgical decompression. Leg and back pain, as well as disability scores, at 18 weeks were improved in the surgery group, but to a non-statistical level. There were 4 serious adverse events in the surgery group and none in the steroid group.
So it seems that surgery may be a little more effective for symptoms, but a little riskier and more expensive. Transforaminal intraepidural injection should at least be considered as a first invasive treatment option before surgery. However, going straight to surgery may be reasonable in certain cases [16].
Surgical techniques for herniated discs
Currently, there are different options such as disc arthrodesis or fusion surgery, which consists of fixing or immobilizing two or more vertebrae to keep them together permanently, or disc arthroplasty or ADR (Artificial Disc Replacement), which consists of replacing the damaged disc with an artificial one [17].
According to Valls, et al. [16] in relation to herniated discs, the gold standard surgical treatment today in 2020 is microdiscectomy (Figure 5).
Also known as percutaneous microdiscectomy, lumbar microdiscectomy is a surgical technique to relieve pressure on nerve roots or the spinal cord. This pressure can occur due to the disc when there is a hernia or due to bony protuberances.
Figure 5 shows a step-by-step demonstration of what is now considered gold standard surgery for the treatment of herniated discs.
According to Wilby, et al. [21], the doctor inserts a guidewire through a small incision to locate the affected disc in the spine. The doctor uses a fluoroscope, which displays X-ray images in real time, to ensure that he or she aligns the path to the correct herniated disc. The surgeon passes a series of dilation tubes over the guidewire, pulling the tissue apart to reach the vertebrae. Once they have access to the herniated disc, the surgeon removes the guidewire. The tubular retractor, through which your doctor will perform the surgery, slides over the dilation tubes. The doctor positions it on the bone surface.
He then removes all the dilation tubes. A surgical light and a small camera allow the doctor to see through the tube. The doctor uses special surgical instruments, passed through the tube, to remove bone and soft tissue and access the spinal canal. The surgeon uses a nerve retractor to gently pull the nerve away from the herniated disc. Using small surgical instruments passed through the tubular retractor, the doctor removes the herniated portion of the disc. He then clears the area sufficiently to allow the nerve to return to its normal position [21].
Finally, the surgeon removes the tubular retractor, which allows the body tissue to close around the surgical site. Since the incision is small for a microendoscopic discectomy, only a small dressing is needed to close the superficial wound. Although you can return home after a period of observation, you need to rest and heal. As the surgical wound heals, you can return to normal daily activities at home. Depending on your profession, you may be allowed to return to work within one or two weeks [21].
Endoscopic spinal surgery (video surgery)
Endoscopic spinal surgery is a modern video-assisted intervention technique. It has minimal tissue aggression, less dissection, less bleeding, a lower percentage of infection and faster recovery. The incision has an average length of 1 cm, the procedure is carried out with an infusion of saline solution and the images are projected onto an external monitor. It can be performed under sedation or general anesthesia with a medical duration of 90 minutes [6].
Most of the time, the patient is discharged the same day or the next day. In addition, the patient is allowed to walk in the immediate post-operative period [22].
There are other types of surgery already established in the treatment of herniated discs. Some of these are more invasive, as shown in Figure 6.
Surgical risks
Complications are rare, less than 3% of cases. However, as with any surgical procedure, there is the associated anesthetic risk, the possibility of infection and problems with healing. In relation to the surgical procedure specifically, neurological injury (damage to the nerve/nerve root) and cerebrospinal fluid fistula (loss of cerebrospinal fluid) are possible complications that are rarely observed [22].
The patient's clinical condition and associated diseases, such as obesity, diabetes and smoking, for example, as well as proper post-operative care influence this risk.
Final Considerations
Surgical and conservative treatments had beneficial long-term effects on sciatica symptoms in patients with lumbar disc herniation. Compared to conservative treatment, surgical treatment relieved low back pain more quickly, but no relevant clinical difference was observed after 3 months. Surgical treatment may therefore be attractive for patients with debilitating pain symptoms who are looking for rapid relief or who have not achieved satisfactory improvement with conservative treatment.