International Journal of Healthcare Systems Engineering
(ISSN: 2633-8939)
Volume 1, Issue 1
Research Article
DOI: 10.35840/2633-8939/7203

Article Formats
Assessment of Obstetric Fistula and Factors Associated among Women admitted to Jimma Medical Center, South West Ethiopia
Table of Content
Figures
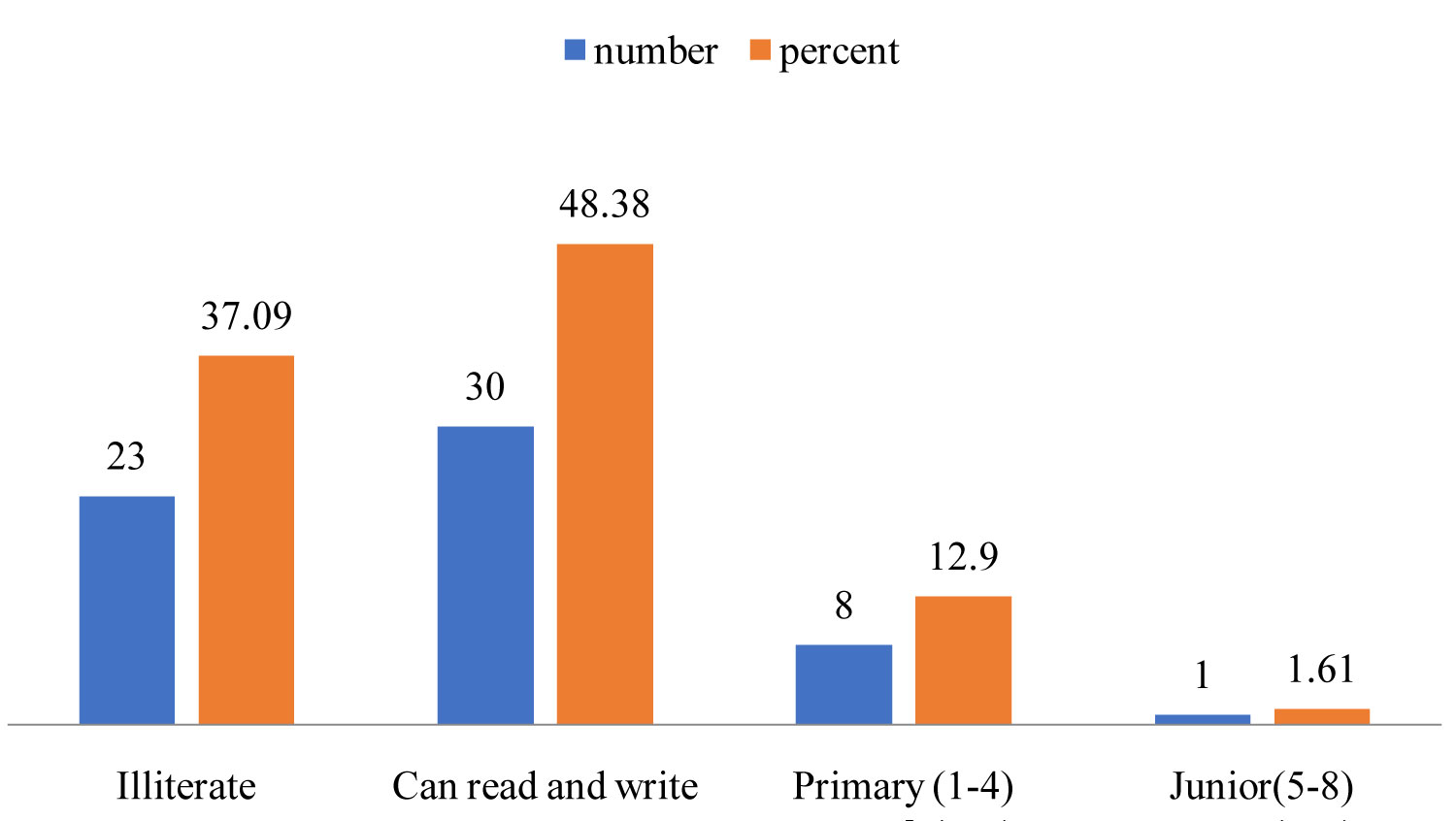
Figure 1: Educational status of women with...
Educational status of women with obstetric fistula at JUSTH southwest Ethiopia, April, 2016.
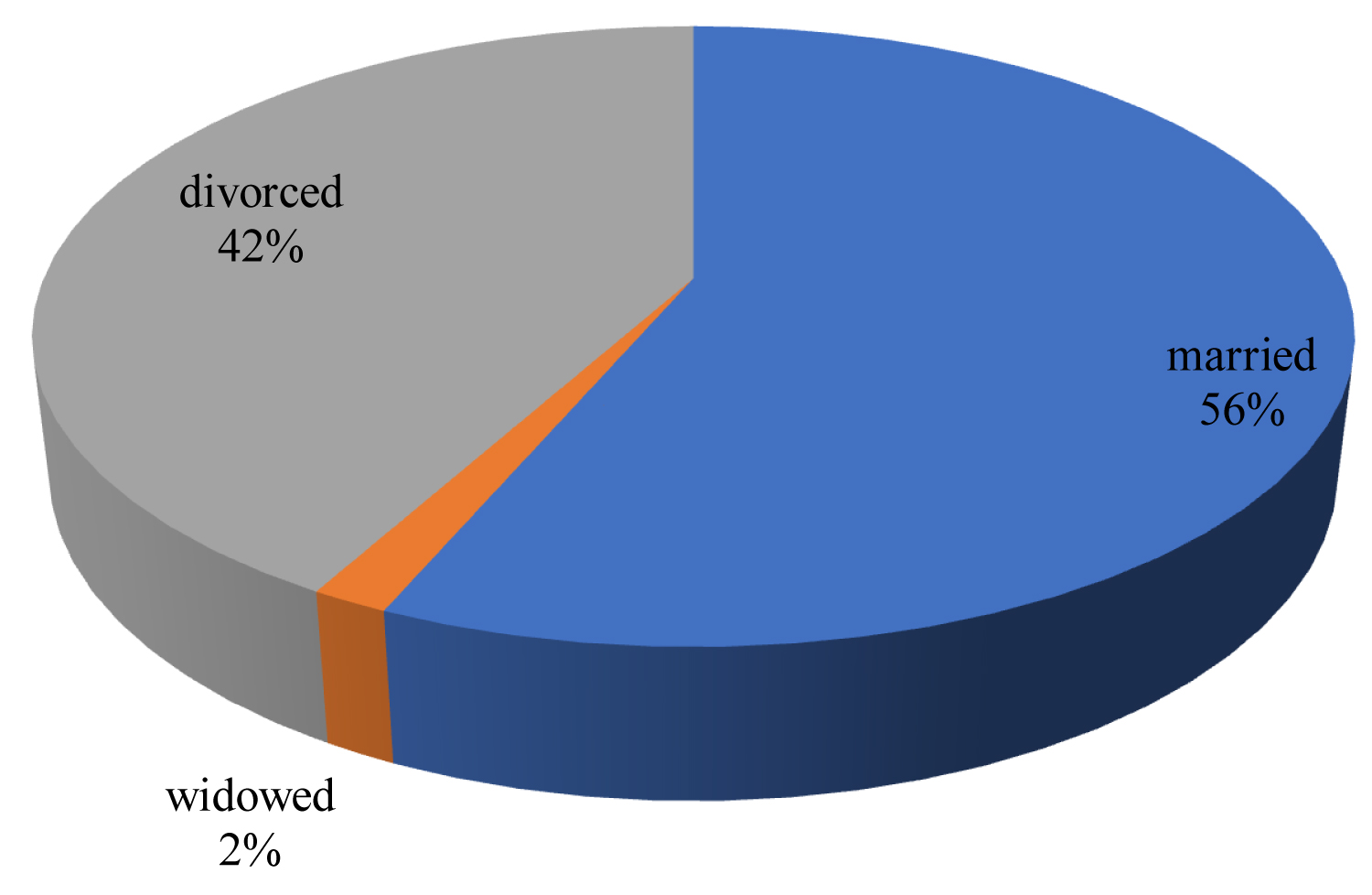
Figure 2: Marital status of women with obstetric...
Marital status of women with obstetric fistula at JUSTH southwest Ethiopia, March, 2016.
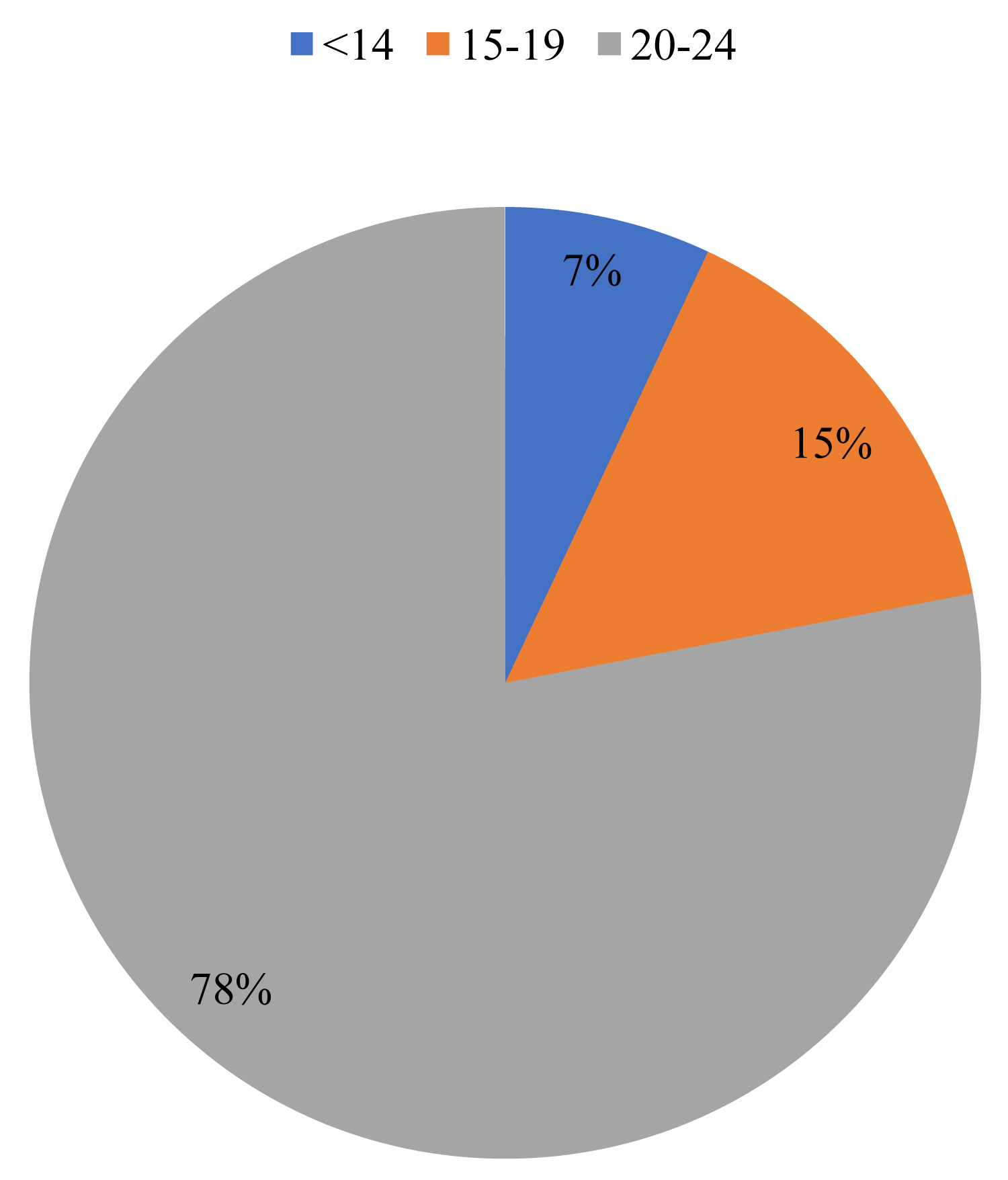
Figure 3: Age at first marriage of women with...
Age at first marriage of women with obstetric fistula at JUSTH Southwest Ethiopia, March, 2016.
References
- AAFH (2006) Obstetric fistula in rural Ethiopia.
- Holme A, M Breen, C Macarthur (2007) Obstetric fistulae: A study of women managed at the Monze mission Hospital, Zambia. BJOG 114: 1010-1017.
- Wall (2006) Obstetric vesicovaginal fistula as an international public-health problem. Lancet 368: 1201-1209.
- Fistula foundation (2011) what is fistula? HH//www fistula foundation 04.
- Addis Ababa (2010) Hamlin fistula Ethiopia, annual report of 2010 report. 3-13.
- WHO (2006) Department of making pregnancy safer. Obstetric fistula guiding principle for clinical.
- (2006) Uganda Bureau of statist and role macro.
- Hilton P (2003) Vesico-vaginal fistulas in developing countries. Int J Gynaecol Obstet 82: 285-295.
- Muleta M (1997) Obstetric fistula retrospective study of 1210 cage at AAFH. J Obstet Gynecol 17: 68-70.
- Danso KA, Marty JO, Wall LL, Elkins TE (1996) The epidemiology of genitourinary fistula in Kumasi, Ghana, 1997-1992. Int Urogynecol J Pelvic Floor Disfunct 7: 117-120.
- WHO obstetric fistula A review of available information maternal health and safe Mather hood program WHO /MCM/MSM/91: 5.
- MOH (2007) Health and health related indicators planning and programming department. Addis Ababa Ethiopia.
- AAFH (2010) Ethiopian road authority and world bank Ethiopia.
- Kelly J, Kwast BE (1993) Epidemiologic study of vesicovaginal fistulas in Ethiopia. Int Urogyncol J 4: 278-281.
- RJ Cook, BM Dicken, S Syed (2004) Obstetric fistula: The challenge to human rights. Int J Gynaecol Obstet 87: 72-77.
- Creanga AA, RR Genardy (2007) Obstetric fistulas: A clinical review. Int J Gynecol Obstet 540.
- Browning Andrew (2004) Obstetric fistula in Ilorin Nigeria. PLoS Med 1.
- Muleto M (2004) Socio demographic positive and obstetric experiences of fistula patients manage at AAFH. Ethiop Med J 42: 9-16.
- (2009) Hamlin fistula international fast facts and FAQs about obstetric fistula AAFH.
- Dekidder D, Badlani GH, Browning A, Singh P, Wall LL. Fistula in developing world.
- Semere, Nour NM (2008) Obstetric fistula: Living with incontinence and shame. Rev Obstet Gynecol 1: 193-197.
- Woaldijik K (2004) The immediate management of fresh obstetric fistula. Am J Obstet Gynecol 1991: 795-799.
- Wall LL, SD Arrowsmith, ND Briggs, A Browning, A Lassey (2005) The obstetric vesciovageinal fistula in the developing world. Obstet Gynecol 60.
- Vagenderhuysen C, Prual A, Ould el Joud D (2001) Obsteric fistula incidence estmates for sub-Saharan Africa. Int J Gynaecol Obstet 73: 65-66.
- (2005) Ethiopian demographic health serves 2005.
- Muleta M, Fantahun M, Tasfaye B, Halmin EC, Kennedy RC(2007) Obstetric fistula in rural Ethiopia. East Afr Med 84: 552-533.
- Asbahahaile (2004) Fistula: A socio economic problem in Ethiopia. Med J 21: 71-77.
- Tahzib F (1983) Epidemiological determinant of VVF. Br J Obstet Gynaecol 90: 387-391.
Author Details
Bikila Dereje* and Elisabeth Abebe
School of Nursing and Midwifery, Jimma University, Ethiopia
Corresponding author
Bikila Dereje, MSc, School of Nursing and Midwifery, Jimma University, Ethiopia.
Accepted: September 28, 2019 | Published Online: September 30, 2019
Citation: Dereje B, Abebe E (2019) Assessment of Obstetric Fistula and Factors Associated among Women admitted to Jimma Medical Center, South West Ethiopia. Int J Healthc Syst Eng 1:003.
Copyright: © 2019 Dereje B, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background
Obstetric fistula is an injury that occurs during prolonged and obstructed labor causing tissue damage to organs inside the pelvis and result in urine and Fecal incontinence or both. It remains a major public health problem in areas where unattended obstructed labor is common.
Methods
An institutional based cross sectional study design was used from February 1 to March 30-2016 to assess obstetric fistula and its associated factors among women. Convenient sampling technique was used for total sample size. Data was collected using structured interviewed questionnaire by 3 trained data collectors. Descriptive statistics was computed to summarize the data.
Result
The total of 62 women was admitted to JUSTH gynecology ward from Feb-Apr 2013. Out of the total respondent 90.32% were developed Vesicovaginal fistula, 22.25% were developed Rectovaginal fistula and 3.2% were developed Recto-vesicovaginal fistula. Majority of the respondents were from the rural area and 50% were in age group 20-24. 66.12% of the respondents had no regular antenatal care follow-up. Among the respondents 87.09% were primiparous. About 56.45% of the cases were caused by obstructed labor and 22.58% were caused prolonged labor.
Conclusion
Generally, prevention is better than cure. Preventing and managing fistula will contribute to achieving improving maternal and child health.
Keywords
Obstetric fistula, Women, Ethiopia
Background
Obstetric fistula is an injury that occurs during prolonged and obstructed labor causing tissue damage to organs inside the pelvis and resulting in urine and fecal incontinence or both. obstetric fistula remains a major public health problem in areas where unattended obstructed labor is the common most frequently reported global prevalence of obstetric fistula shows that approximately 2 million women have untreated fistula and approximately 100,000 women developed fistula each year [1].
Others estimate show that as many as 130,000 new cases of fistula are occurring annually in Africa [2] and globally up to 3.5 million women may believing with the condition [3].
In Ethiopia 9000 women develop fistula each year [4]. There are only 1477 fistula repaired in the year 2010 in all treatment centers including the main hospital in Addis Ababa [5] obstetric fistula makes lives of many young women difficult in developing countries. It is widely known that there are physical problems and co morbidities associated with fistula. Obstetric fistula accounts for 8% of maternal death worldwide with millions more girls and women's living with shame, isolation and poverty because of stigma related to their condition [6].
Although almost no population based surveys on fistula have not yet been under taken and data remains scarce [6].
Estimate suggested that at least 3 million women in poor countries have untreated VVF and that 30,000-130.000 new cases develop each ear in Africa alone [3]. In Ethiopia alone an estimated 0.25% of total population of women suffer with untreated obstetric fistula the vast majority of obstetric fistula cases living in resources poor countries, and almost all of these injurers could have been avoided if timely and competent obstetric care was available, accessible and affordable [7]. Obstetric fistula a devastating medical condition consisting of abnormal opening between vagina and bladder and vagina and rectum resulting from helpless obstructed labor and prolonger labor [6].
In research limited setting women takes various barriers in accessing health care, lack of knowledge to recognize pregnancy and labor complication, powerlessness to seek care distance from facility lack of transport and un affordable cost of transport low expectation of care they desire, serious shortage of medical supplies and equipment and particularly trained personnel further undermine the time line and quality care they receive as a result they often remains suffer from obstetric fistula for years or decades [8].
Statement of the Problem
The world health organization estimates that there are at least 2 million women living with obstetric fistula and annual incidence of 50,000 to 100,000 cases in the world [3].
Obstetric fistula constitutes serious threat to the productive performance of women in Ethiopia the principle cause of obstetric fistula in developing countries like Ethiopia is prolonged obstructed labor beyond the reach of medical help [9]. According to the work done by Dan so, et al. 2004 in kumas 150 out of 157449 delivers resulted in fistula due to obstetric complication of these 73.8% occurred because of prolonged obstructed labor and about 25% was related to early marriage (age < 18 years) [10].
Access to a health institution is a major problem of fistula patients, chiefly because of long distance to reach care, poor transportation and lack of money and because of parturition is regarded as something that can be managed at home [11].
Ethiopian MOH reported that 86.7% of the Ethiopian population has access to primary health care service [12]. Despite the relatively better primary health service coverage available health service utilization rate is very low in Ethiopia hence the country has one of the lowest ANC (52.1%) postnatal care (16.4%) coverage through progressive increasing every year [13].
A study conducted among 30,000 treated case from Addis Ababa fistula hospital over 33 years indicated that 97.4% of the age of the cage was caused by obstructed labor out of which 63% of them were during first child birth [14].
Another report from Ghana identified obstructed labor as cause of fistula in 91.5% case and difficult gynecological surgery in the remaining 8.5% of the cases [12].
Typical fistula patients in Ethiopia are young girls who are married in their early teens to farmers, to illiterate or no education. The girls are given heavy task at home and poorly educated. They have no access to health institution during pregnancy and labor and helped during labor at home. Then deliver dead baby after being in a labor for days. Although obstructed labor kills many of these girls, the survivors develop urogenital fistula because they excluded from their social life they often whish death [11].
Structured interview of 639 fistula patients treated at AAFH between may-Jun 1999-2000 resealed that the mean age of fistula patients at presentation to hospital was 22.7 years, mean age at 1st marriage was 14.7 years [11].
In developing countries, women who are affected by obstetric fistula don not necessarily have full agency over their bodies or their house holds rather their family members or their husband's. Have control in determining the health care that the women receive [14]. Women's family may refuse male doctors, but female doctors may be Unavailable this barring women from prenatal care [15].
Despite the AAFH and five outreach centers dedication to treat women with fistula and massive community awareness activities from promoting treatment, there were only 1477 fistula case repaired in the year 2010, only 16.4 of new patients [5] clearly many women are not seeking treatment as soon as they develop fistula. The reason for delay in seeking treatment is not well known [6]. Therefore, the purpose of this study will be to investigate obstetric fistula and its contributing factors.
Literature Review
Obstetric fistula is a medical condition in which a fistula (Hole) developed between cither the rectum and vaginal or between the bladder and vagina after severe or failed child birth, when adequate medical care is not available [16]. It is considered as disease of poverty because of its tendency to occur in women in poor countries who do not have health resources comparable to developed nations [17].
Until the end of the 19th century and even in early years of 20th century fistula of birth canal from obstetric cause were common diseases (disasters) in Great Britain Europe and USA even though disappearance of obstetric fistula in England Europe and USA by 1920 year [18]. Nowadays obstetric fistula becomes a history in developed world. It used to be a health challenge in those nations late in the 19th and early 20th century [19]. The improvement in the general obstetric care and universal access to emergency obstetric care helped to eliminate obstetric fistula from North America and Europe [20].
The majority of reports concerning fistula came from Africa where early marriage and child bearing are most common [11]. In Africa a number of studies show that 50-80% of women are under the age of 20, with the youngest patients being 12 or 13-years-old, when they are given in marriage [21] and they start bearing of child before physical development is complete this contribute to CPD [13,21].
In sub-Saharan Africa the incidence of obstetric fistula has been estimated to be about 124 cases per 100,000 deliveries in rural areas compared with virtually no cases in major cities [22].
Like many other women in remote areas of poor countries, most women who develop fistula give birth at home without assistance from skilled birth attendants [22].
Traditional practice of early marriage contributes to risk of obstetric fistula. In parts of sub-Saharan Africa and south Asia, where obstetric fistula is most common women are often marry as adolescent, sometimes as young as ten years of age and may become pregnant immediately before their pelvis are full developed for child bearing [23]. In Ethiopia and Nigeria, for example our 25% of fistula patients had become pregnant before the age of 15 and over 50% had become pregnant before the age of 18 years [23].
Women with fistula are often small and short an indication for pelvic immaturity or CPP. They are also usually young, illiterate and poorly educated. Marriage and cursive pregnancy mostly occur before age of 20 years [24]. In Zambia, a study of 259 women with obstetric fistula at Monza mission Hospital found that median age at marriage was 22 years. Delays in receiving emergency obstetric care were experienced at home (67.5%) and at clinics (49.4%) usually due to transport difficulties. About 89.1% of women delivered in health facilities, 50% did not complete primary education [24].
According to Ethiopian demographic health survey, 4% of the women aged 15-49 reported to have obstetric fistula [2]. The analysis of 2005 EDHS data has also shown that the majority of women suffering from obstetric fistula (56.7%) are living in union, one third had obstetric fistula reaching at age. Of 24, more than 2/3 of the women suffering from obstetric fistula are residing in a rural area, 79.6% had their first intercourse before the age of 19 years; and the average age at first marriage among those women is 16.5 years. Additionally, it was indicated that 50.9% of them had no formal education Most of them (55.6%) had No ANC and 86% of them had delivered at home.
In short, the analysis of EDHS 2005 has shown that there is significant association of fistula status with education of women, wealth index, and place of delivery place of residence and use of ANC [25].
A study conducted in Ethiopia, Gondar public health hospital (1999) slowed that 50% of women were aged between 15-20 years and their marriage had been arranged by their parents at age as young as 5 years with mean marriage of 11.5 years [26].
Even though some operations which are used to terminate difficult of labor may cause obstetric fistula as many studies showed the majority of them are due to obstructed labor and prolonged labor [26,27] which lead to damage to pelvic organ the immediate consequence of such damages are urine and fecal in continence and excoriation of vulva from the constant leaking of urine and faces [13].
Age, parity and rape the most common cause of VVF in community given marriage at age before menarche the majority of study in Africa show that 50-80% of women suffering from fistula are primiparous and this percentage is as high as 85% in Sudan and Ethiopia [13,28] the proportion of primiparous who suffer from fistula in Asia varies from about 30% in some parts of India to as high as 85% in Pakistan [26].
Of the 18 obstetric fistula patients in Haile Asbaha study (1999), only six women had been delivered at hospital or clinic and this was only after prolonged obstructed labor only half of them had receive some advice from traditional birth attendant about pregnancy [26].
Harmful traditional practice is responsible for 6-13% of obstetric fistula including gishiri cutting in Northern Nigeria [17].
Methods
An institutional based cross-sectional study design was carried out from February 1 to March 30, 2016 to assess obstetric fistula and its contributing factors among women admitted to JMC.
All women admitted to fistula unit of gynecology ward who were willing to participate in the study were included. Clients who were admitted to other gynecology unit except fistula in gynecology ward who were not willing, had mental problem and cannot communicate.
Since the total number of study population was manageable, all women admitted to gynecology ward (fistula unit) during the study period, no need of calculation for determining the size of study population. Convenient sampling technique was used to take study participants. The data was collected using pretested structured questionnaires. A face to face interviews and record review was conducted by using both closed and open ended questionnaires.
The collected data was checked for internal consistence and processed by using electronic calculator for compilation, summarization and comparison of data. Frequent counts and cross tabulations were used.
The quality of data collection process was monitored by giving clear instruction to the data collectors. Pretest was done prior to data collection period to check reliability of instrument. The collected data was checked and rechecked by the principal investigator and a necessary correction was made each day. Unclear question was briefly explained by using respondent's native language during the actual data collection periods.
Ethical approval was obtained from Institutional Review Board Institute of Health of Jimma University. Following the approval, Official letter of co-operation and support was written to Jimma University specialized hospital from Institute of health science. After getting permission from these hospitals, ethical issues within the study were taken into consideration during the study.
Limitation of the Study
There is scarcity of reliable data on obstetric fistula. National and local prevalence are not well known. Since the study was institutionalized, that might undermine generalization of the result to general population. The study was conducted in the hospital that does not represent a great majority of rural population (community).
Due to lack of complete recorded documents and shortage of time, it was impossible to perfume Retrospective study.
Results
A total of 62 women were admitted to Jimma University Specialized hospital from February-March 30.2016. Out of total respondent, 56 (90.32%) were developed VVF, 14 (22.25%) were developed RVF and 2 (3.2%) were developed RVVF.
Majority of the respondents, (74.19%) were come from rural area and in the age group 20-24 yrs (50%) followed by 25-29 yrs (17.74%). The mean age of the women at the time of study was 26 yrs. Among total respondents, 67.74% were Oromo in ethnicity followed by 20.96% Amhara. Concerning their religion, 64.51% were Muslim followed by 30.64% orthodox. Regarding to economic status of the respondents, majority of them had no income (83.87%) and 6.45% of respondents got < 18 birr per day. The majority of the respondent was housewife (79.03%) followed by farmer which accounts 12.90% (Table 1).
The finding of this study had shown that 66.12% of the respondent had no ANC follow up. Among the respondent only 33.87% of them had ANC follow up out of this 76.19% women had one times visit. Among the respondent 69.35% women were give birth at home and the rest 30.64% were deliver at health institution.
About 75.80% were in labor for more than two days and 64.51% of the women were assisted by NTBA. Only 30.64% of the women were assisted by health professionals. Regarding the outcome of the labor 77.41% were still birth (Table 2).
As indicated in Table 3 urine incontinence (87.09%) was the major problem of the respondent followed by fecal incontinence (25.8%). Among the respondent 90.32% had developed VVF, 22.58% developed RVF Regarding parity, 90.32% of the respondents were primiparous followed by multiparous (9.67%). Related to contributing factor 56.45% of the respondent had developed fistula due to obstructed labor followed by prolonged labor (19.35%) (Table 4).
This Figure 1 shows that majority of the respondent can read and write (48.38%) and 37.09% were illiterate.
As indicated in Figure 2 the majority of the respondents were married (56%) and 42% were divorced.
As indicated in the above Figure 3 78% of the respondents were married at age group 15-19 years.
Discussion
This study showed that majority of study population fistula case were from rural areas which is similarly to the finding of EDHS 2005. According to EDHS (2005), 75% of the women suffering from obstetric (fistula) reside in rural areas [25].
Additionally, study the showed that 50% of the respondent were in age group 20-24 years. This is different from the study conducted in Gonder public health hospital which had shown that 50% of women with obstetric fistula were in age group 15-20 years [26]. This variation might be due to application of Ethiopian civil code for marriage of female and improvement of grills educational status.
About 48.38% of women with obstetric fistula can read and write it is different from EDHS2005 which indicate 50.9% of women with obstetric fistula had no formal education [2]. It is different from the study conducted in Zambia which had shown that 50% of women with obstetric fistula were illiterate [24]. This difference might occur due to variation of study period and the effort of government to achieve MDG (education for all).
The study also reveals 83.87% of women with obstetric fistula had no income this finding is similarly with study conducted in AAFH (2006) which showed that 85.4% of women with obstetric fistula had no income.
According to the finding of this study 70.96% of women with obstetric fistula were under 20 years when they were married. Similarly, the number study in Africa showed that 50-80% of women with obstetric fistula were under 20 year when they were married [21]. This indicated that the problem of early marriage is still present. Out of the total respondent 66.12% of women with obstetric fistula had no ANC follow-up their certain variation with EDHS which indicate (55.6%) had no ANC follow-up [26]. This might occur due to size of study population and study period also it could due to lack of awareness about complication of pregnancy, lack transport and lack of satisfaction with quality and quantity of ANC service.
Most of the women with obstetric fistula give birth at home [22]. This study showed that 69.35% of women with obstetric fistula were delivered at home and 64.51% were assisted by NTBA. This is different from EDHS 2005 (86%) women with obstetric fistula had delivered at home [2]. This might be occurring due to awareness created by government about women with obstetric fistula importance of giving at health institution through media and health extension worker. Another study in Zambia, study of 259 women with obstetric fistula at monze mission hospital found that 67.5% women with obstetric fistula were delivered at home [24]. This is almost similar with the finding of this study.
About 87.09% of the respondents were primiparous Majorities of studies in Africa also showed that 50-80% of women with obstetric fistula were primiparous and this percentage is as high as 85% in Ethiopia and Sudan [13]. The proportion of primiparous who suffer from fistula in Asia varies from about 30% in some parts of India and 85% in Pakistan [26]. This might be due to immaturity of pelvic organ in primigravida.
Even though some operation which are used to terminate difficulty of labor may cause obstetric fistula, as many studies showed majority them were caused by obstructed and prolonged labor [26,27]. This study showed that 56.45% case were caused by obstructed labor which was less when compared to study conducted in AAFH in which 97.4% of the case were caused by obstructed labor [14]. The rational might be the improvement of obstetric care and expansion of emergency obstetric care.
Conclusion
In general, the finding of this study revealed that: Majority of women with obstetric fistula were from rural areas. Obstetric fistula occurs in high rate within low economical and educational status of women. Primiparous are mostly at risk to develop obstetric fistula. Most women developed obstetric fistula due to obstructed prolonged labor, age, parity, rape, CPD, and first sexual intercourse were the main contributing factors for obstetric fistula. Lack of many transport and access to emergency obstetric care increase the risk of developing obstetric fistula.
Author Contributions
BD involved substantial contributions to conception and design of the study, data collection, data analysis, interpretation of data and drafting and critically reviewing the manuscript. Likewise EA involved in designing of the study, analysis of the data and critically reviewing the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest
There are no conflicts of interest.
Acknowledgement
First and for most we would like to thank our Almighty God for His help in all walk of our life and for giving us healthy and great help during day and night time to do this study. And also, our great thanks go to all participants of the study for their willingness, genuine information and the time sacrifices.