International Journal of Biomechanics and Movement Science
(ISSN: 2631-5114)
Volume 3, Issue 1
Research Article
DOI: 10.35840/2633-8955/9723

Article Formats
Asymptomatic Rotator Cuff Tears are Associated with Biomechanical Changes Enabling Early Detection before Functional Limitations Present
Table of Content
Figures
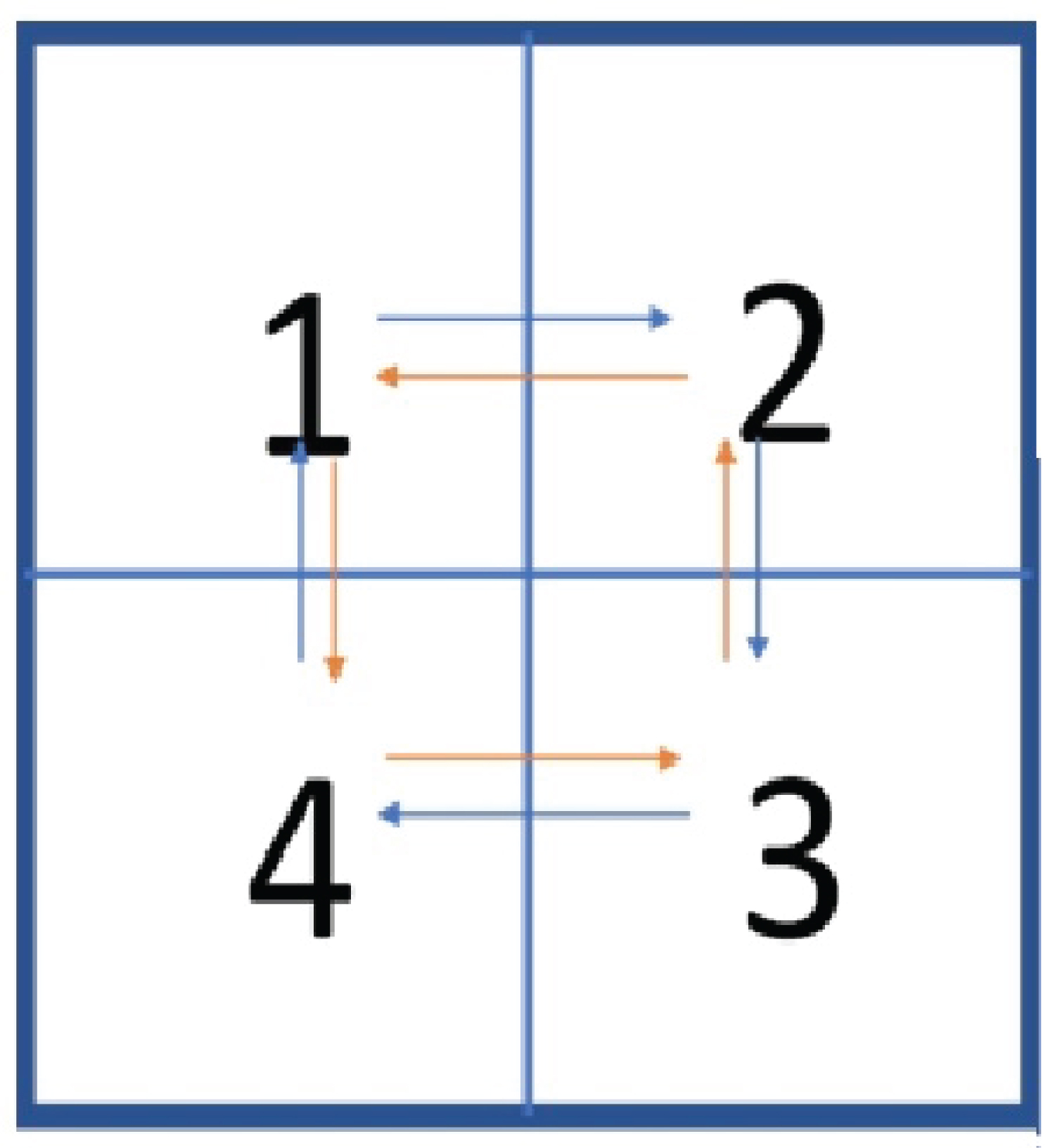
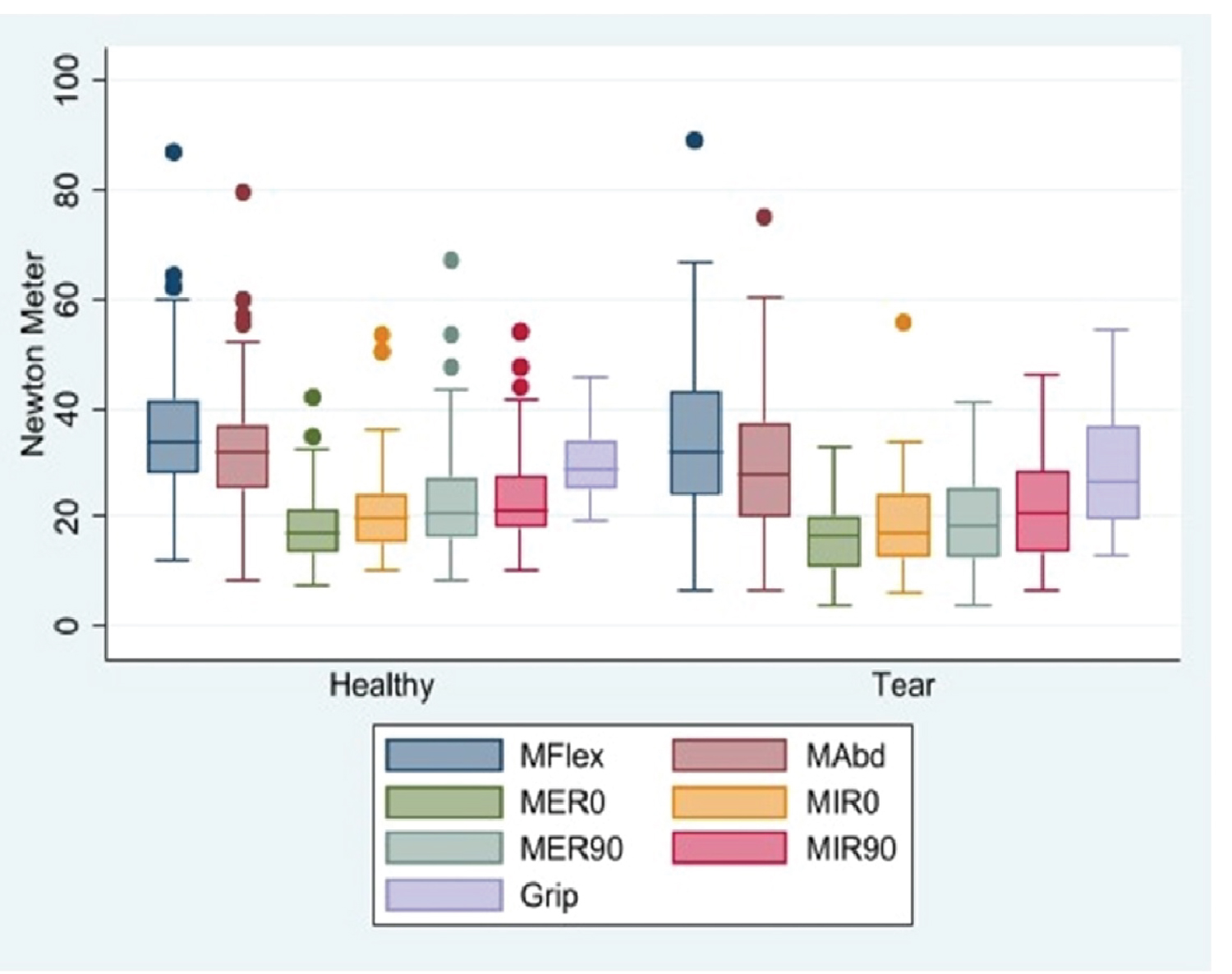
Figure 2: Moment of shoulder in....
Moment of shoulder in different arm positions in two conditions of with and without RCT. Moment = Force × moment arm which means the force measured by dynamometer (newton) multiplied by the distance of shoulder joint to the point of force application (m). M Flex = moment in Flexion, M A bd = moment in abduction, MER 0 and MER 90 = moment in external rotation at 0 degree and 90 degrees of arm elevation respectively, MIR 0 and MIR 90 = moment in internal rotation at 0 degree and 90 degrees of arm elevation respectively.
Tables
Table 1: Demographic information of tear and healthy groups.
Table 2: Mean (Standard Error) of Range of motions measured in degrees. Beta coefficients and p values are obtained from the mixed effect regression models considering age, sex, dominant arm and within participant effects.
Table 3: Mixed effect model for evaluating the effect of tear on the shoulder moments. Age, sex, arm dominance and the within subject effects have been considered in the model.
References
- Mitchell C, Adebajo A, Hay E, Carr A (2005) Shoulder pain: Diagnosis and management in primary care. BMJ 331: 1124-1128.
- Vitale MA, Vitale MG, Zivin JG, Braman JP, Bigliani LU, et al. (2007) Rotator cuff repair: An analysis of utility scores and cost-effectiveness. J Shoulder Elbow Surg 16: 181-187.
- Itoi E (2013) Rotator cuff tear: Physical examination and conservative treatment. J Orthop Sci 18: 197-204.
- Lawrence RL, Moutzouros V, Bey MJ (2019) Asymptomatic rotator cuff tears. JBJS Rev 7: e9.
- Saccomanno MF, Salvatore M, Grasso A, Milano G (2014) Full-thickness rotator cuff tears. Shoulder Arthroscopy. Springer 289-306.
- Yamaguchi K, Tetro AM, Blam O, Evanoff BA, Teefey SA, et al. (2001) Natural history of asymptomatic rotator cuff tears: A longitudinal analysis of asymptomatic tears detected sonographically. J Shoulder Elbow Surg 10: 199-203.
- Kelly BT, Williams RJ, Cordasco FA, Backus SI, Otis JC, et al. (2005) Differential patterns of muscle activation in patients with symptomatic and asymptomatic rotator cuff tears. J Shoulder Elbow Surg 14: 165-171.
- Baumer TG, Dischler J, Mende V, Zauel R, Holsbeeck MV, et al. (2017) Effects of asymptomatic rotator cuff pathology on in vivo shoulder motion and clinical outcomes. J Shoulder Elbow Surg 26: 1064-1072.
- Kijima T, Matsuki K, Ochiai N, Yamaguchi T, Sasaki Y, et al. (2015) In vivo 3-dimensional analysis of scapular and glenohumeral kinematics: Comparison of symptomatic or asymptomatic shoulders with rotator cuff tears and healthy shoulders. J Shoulder Elbow Surg 24: 1817-1826.
- Moosmayer S, Smith HJ, Tariq R, Larmo A (2009) Prevalence and characteristics of asymptomatic tears of the rotator cuff. An ultrasonographic and clinical study. J Bone Joint Br 91: 196-200.
- Keener JD, Steger-May K, Stobbs G, Yamaguchi K (2010) Asymptomatic rotator cuff tears: patient demographics and baseline shoulder function. J Shoulder Elbow Surg 19: 1191-1198.
- Kim HM, Teefey SA, Zelig A, Galatz LM, Keener JD, et al. (2009) Shoulder strength in asymptomatic individuals with intact compared with torn rotator cuffs. J Bone Joint Surg Am 91: 289.
- Langford Z (2015) The four square step test. J Physiother 61: 162.
- Kibler WB, Press J, Sciascia A (2006) The role of core stability in athletic function. Sports Med 36: 189-198.
- Yamamoto A, Takagishi K, Kobayashi T, Shitara H, Osawa T (2011) Factors involved in the presence of symptoms associated with rotator cuff tears: A comparison of asymptomatic and symptomatic rotator cuff tears in the general population. J Shoulder Elbow Surg 20: 1133-1137.
- Dunn WR, Kuhn JE, Sanders R, An Q, Baumgarten KM, et al. (2014) Symptoms of pain do not correlate with rotator cuff tear severity: A Cross-sectional study of 393 patients with a symptomatic a traumatic full-thickness rotator cuff tear. J Shoulder Elbow Surg Am 96: 793-800.
- Unruh KP, Kuhn JE, Sanders R, An Q, Baumgarten KM, et al. (2014) The duration of symptoms does not correlate with rotator cuff tear severity or other patient-related features: A cross-sectional study of patients with a traumatic, full-thickness rotator cuff tears. J Shoulder Elbow Surg 23: 1052-1058.
- Silfies SP, Ebaugh D, Pontillo M, Butowicz CM (2015) Critical review of the impact of core stability on upper extremity athletic injury and performance. Braz J Phys Ther 19: 360-368.
- Gaitini D (2012) Shoulder ultrasonography: Performance and common findings. J Clin Imaging Sci 2: 38.
- Teefey SA, Rubin DA, Middleton WD, Hildebolt CF, Leibold RA, et al. (2004) Detection and quantification of rotator cuff tears: Comparison of ultrasonographic, magnetic resonance imaging, and arthroscopic findings in seventy-one consecutive cases. J Shoulder Elbow Surg Am 86: 708-716.
- De Jesus JO, Parker L, Frangos AJ, Nazarian LN (2009) Accuracy of MRI, MR arthrography, and ultrasound in the diagnosis of rotator cuff tears: A meta-analysis. Am J Roentgenol 192: 1701-1707.
- Vlychou M, Dailiana Z, Fotiadou A, Papanagiotou M, Fezoulidis I (2009) Symptomatic partial rotator cuff tears: diagnostic performance of ultrasound and magnetic resonance imaging with surgical correlation. Acta Radiol 50: 101-105.
- Iannotti JP, Ciccone J, Buss DD, Visotsky JL, Mascha E, et al. (2005) Accuracy of office-based ultrasonography of the shoulder for the diagnosis of rotator cuff tears. J Shoulder Elbow Surg Am 87: 1305-1311.
- Rosa MV, Perracini MR, Ricci NA (2019) Usefulness, assessment and normative data of the functional reach test in older adults: A systematic review and meta-analysis. Arch Gerontol Geriatr 81: 149-170.
- Lovern B, Stroud L, Ferran N, Evans S, Evans R, et al. (2010) Motion analysis of the glenohumeral joint during activities of daily living. Comput Methods Biomech Biomed Engin 13: 803-809.
- Hall LC, Middlebrook EE, Dickerson CR (2011) Analysis of the influence of rotator cuff impingements on upper limb kinematics in an elderly population during activities of daily living. Clin Biomech 26: 579-584.
- Manske RC, Jones DW, Dir CE, LeBlanc HK, Reddy MA, et al. (2021) Grip and shoulder strength correlation with validated outcome instruments in patients with rotator cuff tears. J Shoulder Elbow Surg 30: 1088-1094.
- Chaudhari AM, McKenzie CS, Pan X, Oñate JA (2014) Lumbopelvic control and days missed because of injury in professional baseball pitchers. Am J Sports Med 42: 2734-2740.
- Waldron JL, McKenney MA, Samuel MN, Girouard TJ, Turner CL, et al. (2020) The use of postural restoration for treatment of chronic rotator cuff pathology: A case report. Int J Sports Phys Ther 15: 832-839.
- Yörükoglu AÇ, Savkin R, Büker N, Alsayani KYA (2019) Is there a relation between rotator cuff injury and core stability? J Back Musculoskelet Rehabil 32: 445-452.
Author Details
Talia Alenabi1*, Omid Ashrafizadeh1, Helen Razmjou2 and Clark R Dickerson1
1Department of Kinesiology, University of Waterloo, Waterloo, Canada
2Holland Orthopedic & Arthritics Centre, Sunnybrook Health Sciences Center, Toronto, Canada
Corresponding author
Department of Kinesiology, University of Waterloo, Waterloo, Canada.
Accepted: March 23, 2023 | Published Online: March 25, 2023
Citation: Alenabi T, Ashrafizadeh O, Razmjou H, Dickerson CR (2023) Asymptomatic Rotator Cuff Tears are Associated with Biomechanical Changes Enabling Early Detection before Functional Limitations Present. Int J Biomech Mov Sci 3:003
Copyright: © 2023 Alenabi T, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Asymptomatic rotator cuff tears are common and understanding their characteristics may help clinicians to recognize this pathology in early stages. The main questions of this study were 1) If the range of motion and strength of shoulders with asymptomatic tears were comparable with the intact shoulders; and 2) If the individuals with asymptomatic tear had deteriorated static and dynamic core balance.
Methods: Both shoulders of 70 participants over age of 50 years and without shoulder pain and dysfunction were evaluated by ultrasonography to distinctintact rotator cuff and asymptomatic tears. Shoulder range of motions and isometric strength in flexion, abduction, internal and external rotations, and grip were evaluated. The static and dynamic core balances were also assessed by standard tests. Regression models were used to identify the significant differences between groups.
Findings: 33% of the shoulders had partial or full thickness rotator cuff tears. Shoulders with tear had significantly lower range of motion in flexion, abduction and reaching back posture (internal rotation), p ˂ 0.05. Although statistically non significant, the mean shoulder moments in the tear group were generally lower than the intact shoulders for all postures but grip. Individuals with and without asymptomatic rotator cuff tears had comparable static and dynamic core stability (p > 0.05).
Interpretation: This study suggests that individuals with asymptomatic rotator cuff tears may have difficulties in performing tasks that need an extreme range of motions or exhibit a small decline in isometric shoulder strength. Clinicians who work with the elderly population should consider these early manifestations of rotator cuff diseases.
Keywords
Rotator cuff tear, Asymptomatic shoulder, Shoulder moment, Shoulder range of motion, Core balance, Grip strength
Introduction
Shoulder pain is the third most common cause of musculoskeletal consultation in primary care [1], and rotator cuff pathologies are the main cause of chronic shoulder pain. According to 2010 US census data [2], close to 6 million US citizens have rotator cuff tears (RCT) with reports of 75,000 to 250,000 surgical repairs annually. The occult nature of RCTs complicates their prevention; RCTs can be completely silent prior to the presentation of debilitating symptoms. Medical reports suggest that for each symptomatic tear encountered in a medical service, there are 4 more cases with symptoms and 10 more asymptomatic cases tear in society that go undetected [3]. Indeed, prevalence of asymptomatic partial-thickness and full-thickness tears vary from 8 - 40% and 6 to 46% respectively [4]. Risk of asymptomatic RCTs increases with age, and patients who are being treated for pain for an RCT may have an asymptomatic tear in the contralateral shoulder [4]. Asymptomatic tears typically do not remain silent indefinitely, with up to half of these injuries becoming symptomatic within ~3 years [5,6].
In terms of clinical presentations of asymptomatic tears, the literature shows inconsistency in range of motion and strength as compared with symptomatic tears. While minor deficits in elevation have been reported in patients with asymptomatic tears [7], others have reported no difference between groups with asymptomatic tears and intact tendons [8-11]. The strength related differences are also inconsistent in the literature [12,13]. As a result, the extent to which an asymptomatic cuff tear affect functional abilities is not clear, nor are guidelines for potential clinical identification of early-stage tears. In fact, the investigations performed on strength and range of motion of shoulders with asymptomatic RCT come with important caveats. First, many of these studies only focused on the full thickness RCTs, while there are sufficient evidence suggesting that the severity of patient’s symptoms does not correlate to the tear type [14,15]. Second, some studies examined the asymptomatic shoulders of individuals with one symptomatic shoulder. These individuals might be predisposed to deficits compared to completely asymptomatic people. Third, the strength was measured only in certain shoulder postures and some common postures such as grip were ignored. Forth, in some studies, the age range of study population was considerable, and the potential independent influence of age or sex on biomechanical deficits was left unaddressed. In addition, while there are some studies suggesting that deficit in core neuromuscular balance may affect the risk of shoulder injuries in athletic population [16], such studies have not been conducted in non-athlete people. Understanding the characteristics of asymptomatic RCT is important because hypothetically, interventions that help to prevent progression of this condition are likely more effective before symptoms become severe. Studies on asymptomatic RCT may help clinicians and researchers to approach and identify this condition early in its progression.
The primary objective of this study was to compare the range of motion and maximum isometric strength moments of the shoulder in various postures between shoulders with asymptomatic partial or full thickness rotator cuff tears and those with an intact rotator cuff. Moreover, this study aimed to evaluate if static and dynamic core balance measurements differed between these two groups. It was hypothesized that people with asymptomatic rotator cuff tear would have some deficits in strength and range of motion in the affected shoulders. It was also expected that they would have lower core balance scores compared to the ones with intact rotator cuff.
Methods
Participants
Seventy volunteers over age of 50 years, without any history of shoulder pain, injury, trauma, or surgery were recruited from the Waterloo Research of Aging Pool (WRAP) population and local communities. The exclusion criteria included history of neuromuscular diseases, neurovascular accidents, or systemic diseases such as rheumatoid arthritis. Those who reported receiving physiotherapy treatments for shoulder pain during the last 6 months were also excluded.
The research was approved by the ethics committee of the local institute. Participants received an informed consent form before arrival and all the research process were explained by one of the researchers before signing the consent form. All subjects were interviewed by a researcher and completed a number of self-report surveys and objective functional measures.
Ultrasonography examination
The distinction between healthy and asymptomatic shoulders was made by ultrasound studies. A sports medicine physician with more than 10 years’ experience in shoulder ultrasound examination evaluated both shoulders of the participants. Ultrasonography (SonoSite M-Turbo, L38e) using a 12-MHz linear-array probe was performed in the longitudinal and transverse views of the supraspinatus, infraspinatus, subscapularis and biceps tendons in the previously defined positions [17]. Several studies have shown that ultrasound can reveal comparable results to MRI in detecting cuff pathology [18-21], and it is a valid tool to detect present or absent of tear.
Individuals and shoulders with an intact rotator cuff were grouped as the “Healthy” and those with either partial or full thickness tear in at least one tendon were placed in the tear group.
Self-report questionnaires
This included the “Quick Disabilities of the Arm, Shoulder and Hand” (Quick-DASH) questionnaire, the “American Shoulder and Elbow Surgeons (ASES)” Patient Assessment Forms and a general questionnaire asking about smoking habit, comorbidities, history of fall, and lifestyle parameters. The participants could either receive the electronic version of questionnaires to complete at home or write their responses on the hard copies in person.
Objective measurements
Active Range of Motion (RoM): Active RoMs were measured bilaterally using a goniometer during full shoulder flexion, abduction, and external rotation while the arm was close to the body in standing position. For measuring the RoM in internal rotation, the participants were instructed to put their thumbs between the two scapulae as high as possible. The distance between the thumb and the C7 was recorded. Internal and external rotations were also measured in 90° of arm abduction in supine position. All the measurements were performed twice, and the highest RoM was used for subsequent analysis.
Isometric moments (force × moment arm): Using a measuring tape, the moments arms were measured as follows: the distance between the acromion to the wrist (for flexion and abduction moments) and the distance between the lateral epicondyle of the elbow to the wrist (for internal and external rotation moments). To identify the point of measurement at the wrist, a line between the two styloid process of the wrist was drawn and the handle of the dynamometer was placed tangent to this line. The midpoint between the upper and lower borders of the handle was identified for the above measurements.
Using a manual dynamometer (ErgoFet, Hoggan Scientific, USA), the strength of both shoulders was measured in 90° flexion, 90° abduction, internal rotation (0° and 90°) and external rotation (0° and 90°) in the positions explained for RoM measurements. The handle of the dynamometer was placed on the wrist above the line between the two styloid processes. The participant was instructed to push against the dynamometer while it was fixed in a static condition by a young strong researcher. The participants could do a few rehearsals before actual measurement. Manual grip dynamometer was also used to record grip strength bilaterally, while the participant held the dynamometer close to their body with a stretched arm, applying maximum squeezing force to the handle. All measurements were performed twice, and the highest score was used for analysis. To calculate moments, the strength scores (Newtons) were multiplied by the moment arms (m).
Balance tests for evaluating the static and dynamic stability: Functional Reach Out Test (FRT) [22] was used for evaluating the static balance. Participants were asked to stand next to, but not touching, a wall by their non-dominant side while their body was exactly closes the 0 point of a ruler attached to the wall. They were asked to stretch the arm that was closer to the wall at 90 degrees of shoulder flexion with a closed fist. The location of the third knuckle was recorded. Afterward, the participants were advised to reach as far as they could forward without taking a step. The position of the third knuckle was recorded in this position too. Scores were determined by calculating the difference between the start and end position is the reach distance.
Four Steps Square Test (FSST) [23] was used for evaluating dynamic balance. Four squares (30 × 30 cm) were made on the floor using a color tape set up like a cross (Figure 1). Participants were instructed to step in each square as fast as possible with the following sequences: 1,2,3,4,1,4,3,2,1. Participant had to complete the sequence without touching the tapes and both their feet must have contacted the floor in each square. The sequence was demonstrated to the participants, and they could practice. Two FSST were completed with the best time taken as the score.
The examiner who performed the measurements was blinded to the tear condition.
Statistical analysis
Participants were divided in two groups: 1) Those with both healthy shoulders, and 2) Individuals with either partial or full thickness tear in at least one shoulder. Age, BMI, DASH and ASES scores were compared in two groups using T test or test. The FRT and FSST were also compared using linear regression that considered the effect of age and sex. For the rest of the analysis, we included all the healthy shoulders in one group (94 shoulders) and all the shoulders with tear in another group (46 shoulders). A mixed effect linear regression model was developed to consider the effect of age, sex, arm dominance as well as the within participant effect. Using this model, the effect of tear on range of motions and isometric moments were evaluated. The Stata/IC 16 software was used for data analysis and the significance level was set at p < 0.05.
Results
Thirty-one participants had tear in either one shoulder (16 participants, 14 right, 2 left) or both shoulders (15 participants). The group differences are demonstrated in Table 1. Among 46 shoulders with RCT, 29 tears were only in supraspinatus, 1 only in infraspinatus, 8 in both supraspinatus and infraspinatus, 8 shoulders had tear in all three tendons. Partial tears accounted for 28 shoulders, while 16 shoulders had small to medium full thickness tear (< 3 mm to 3-5 mm respectively) and only two shoulders showed large tear (> 5 mm).
Range of motion
The information regarding the range of motions have been summarized in Table 2. Shoulders with RCT had significantly lower RoM in flexion and abduction and the distance of the thumb to C7 was higher in internal rotation posture. The effect of sex was only significant for the internal rotation at 0° of arm elevation (p < 0.001), while the effect of age was significant for flexion and external rotation at 90° of arm elevation, (p > 0.05).
Moment/strength
The measurements of shoulder moments in different postures have been presented in Figure 2.
There were no significant differences in shoulder strength between healthy and RCT shoulders, except for the grip strength that male individuals with tear showed significantly higher values (Table 3). Shoulders in tear group showed larger variability in their strength measurements. The effect of sex and age were significant for all the measurements while the effect of arm dominance was not significant (p > 0.05).
Balance
The crude analysis of the effect of tear on the static and dynamic balance revealed a significant association of tear with the time to complete Four Steps Square Test. However, when the analysis was adjusted for the age and sex, no significant differences in FRT distances (p = 0.5) or FSST time (p = 0.08) were revealed between groups. The mean FRT distance were 35.1 ± 7.1 cm and 34.1 ± 8.6 cm for healthy group and tear group respectively. The mean FSST time was 6.5 ± 1.5 s in healthy group and7.76 ± 2.6 s in tear group.
Discussions
In this study 33% of the shoulders had either partial or full thickness tears, confirming that asymptomatic RCTs frequently occur. The results suggest that shoulders with tear may have some deficit in certain RoMs while their isometric strength can be comparable with the healthy shoulders. In addition, people with and without asymptomatic RCT may have comparable static and dynamic core stability.
Range of motion
Individuals with asymptomatic RCT displayed deficits in certain range of motion in the affected shoulder. The average differences in maximal flexion and abduction were 10.8° and 13.8° respectively. In addition, pathologic shoulders had limited internal rotation when attempting to reach their backs (5 cm less in average). The decline in the range of motion agrees with some researchers such as Kelly, et al. [7] who found approximately 6° less arm elevation in the scapular plane in individuals with asymptomatic rotator cuff pathology. However, these findings contrast with other studies who reported no differences in RoM in healthy and asymptomatic RCT shoulders [8,10]. Differences in measurement methods and evaluated plane of elevation may explain these contradictory findings. Approximately 60° shoulder range of motion is required to perform most daily living activities [24], therefore, although the observed deficit in shoulder range of motion may not impact many routine activities, it could limit tasks or activities requiring an extreme range of shoulder motion such as reaching to a high shelf. An intact rotator cuff tendon is necessary to provide a stable base for shoulder movements in those conditions. This issue was previously explained by Hall, et al. [25] who reported limited shoulder range of motion in a group of elderly with positive impingement tests.
Strength
None of the shoulders with asymptomatic tear had significant differences in isometric arm strength in flexion, abduction and internal and external rotations compared to healthy shoulders. However, the range of strength measurements was wider in the tear group comparedto healthy ones (Figure 2), indicating that certain cases with tear had lower strength measurements. It is in accordance with Kim, et al. [12] who reported no difference in strength at 90° abduction in scapular plane and ER at 0° of arm elevation between asymptomatic shoulders with partial- or full-thickness tear and the intact shoulders, but they found significantly lower abduction strength in the shoulders with massive rotator cuff tears. Baumer, et al. [8] also reported a comparable strength of internal and external rotations at 15° arm elevation in the two groups, and lower strength in 30° abduction and flexion in shoulders with asymptomatic RCT. Posture differences may explain these different results. In addition, the majority of the participants in our study had small to medium size tears only in supraspinatus. The abovementioned studies reported lower elevation strength in the shoulders with a large-to-massive full-thickness rotator cuff tear. The tear characteristics likely explain why our participants showed less weakness in isometric exertions.
Interestingly, this study showed higher grip strength in the asymptomatic shoulders. The interaction effect of gender and tear significantly influenced grip strength, particularly that men with RCT had higher strength values. Therefore, people with asymptomatic RCT probably do not have any difficulty in performing the tasks that need maximum grip effort. This is in accordance with a recent study that reported no relationship between rotator cuff dysfunction and grip strength [26].
Balance
The current study suggests that the static and dynamic balance of individuals with asymptomatic RCT is compatible with individuals with healthy shoulders. Previous studies suggest a potential relationship between poor core control and shoulder injuries [27,28] particularly in athletic populations. These observations suggest that abnormal neuromuscular control in any part of the kinetic chain can influence upper extremity demands, although the causative effects of balance deficit on shoulder injuries are uncertain. No reports exist for FRT and FSST tests performed on persons with asymptomatic RCTs. Clinical reports suggest that core and pelvic stability exercises may decrease shoulder pain associated with rotator cuff ten dinopathy [29,30]. Future studies will reveal if the static and dynamic balances differ in asymptomatic and symptomatic cases with RCT and if balance exercises can affect symptom occurrence in asymptomatic group.
Limitation
The proposed sample size of this study was larger than the numbers reported. Due to Covid19 pandemics, the data collection was stopped in the middle of the study; however, this report still adds to the current knowledge regarding the biomechanical characteristics of asymptomatic RCTs. This study not only provides a more thorough understanding of the effect of asymptomatic RCT on the shoulder range of motion and isometric strength by examining several postures, but also sheds light on the potential association of this asymptomatic condition with grip strength and the static and dynamic balance which were not studied before.
Conclusion
This study confirms that there are differences in shoulder range of motion and strength in shoulders with asymptomatic rotator cuff tear and intact tendon. The findings suggest that unless the tear size is not massive and the shoulder strength is comparable with the healthy condition, the individuals may remain asymptomatic. However, clinicians who work with elderly population should consider the early manifestations of asymptomatic rotator cuff tears such as limited range of motion or small declines in shoulder strength and evaluate the progression of these conditions. Clinical trials are required to reveal if RoM and strength training would decrease the likelihood of symptom occurrence in asymptomatic RCT condition.
Source of Support
This study was supported by MITACS (Grant number: IT11817).
Acknowledgements
The collaboration of Silverberry Genomics Inc. and Shayan Mashatianin grant application, and Jaclyn Kurt and Daniel Fournier in data collection is appreciated.
Ethics Approval
The Office of Research Ethics at the University of Waterloo approved this study. All participants gave written informed consent before data collection began.
Declaration of Interests
None.